Why Does Muscle Pain Spread?
Referred Pain, Peripheral Sensitization, and the Experiment That Showed How Your Spinal Cord Rewires in Minutes
You press on a knot in your shoulder and feel a headache bloom behind your eye. The trigger point is in your trapezius, but the pain is in your skull. This is referred pain, and the mechanism behind it reveals something fundamental about how your nervous system processes muscle injury, and why treating the actual source matters more than chasing the symptom.
- Peripheral sensitization occurs when inflammatory mediators or tissue damage lower the firing threshold of sensory nerve endings, making them respond to stimuli that would normally be painless (Latremoliere & Woolf, 2009).
- In a landmark experiment, injecting a pain-producing substance into one muscle caused spinal cord neurons to develop entirely new receptive fields in distant muscles within five minutes (Hoheisel et al., 1993).
- Referred muscle pain depends on continuous nociceptive input from the original pain site. Block that input with local anesthetic, and the referred pain resolves (Rubin et al., 2009).
- Active trigger points function as peripheral pain generators that can both initiate and maintain widespread pain, including in conditions like fibromyalgia (Staud et al., 2009).
- Two substances are particularly important for generating muscle pain: ATP (via P2X3 receptors) and hydrogen ions (via TRPV1 and ASIC channels) (Mense, 2008).
Pain That Radiates, Refers, or Seems to Move Around?
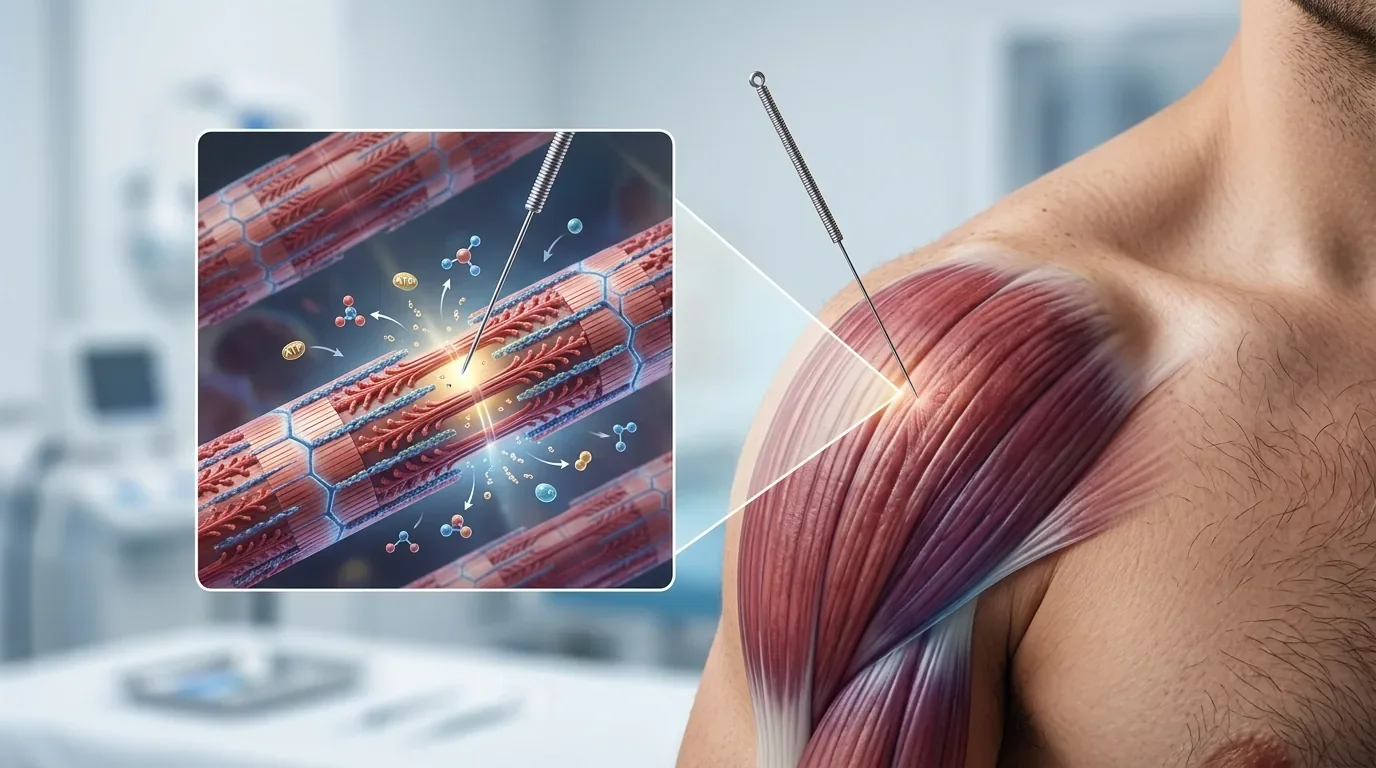
Referred pain from trigger points is one of the most commonly misdiagnosed patterns in musculoskeletal medicine. Our practitioners trace pain to its muscular source and treat it directly with precision dry needling.
Schedule NowWhen Pain Receptors Become Too Sensitive
Under normal circumstances, pain receptors in muscle tissue only fire when a stimulus is strong enough to threaten tissue damage. But when these nerve endings are bathed in inflammatory chemicals or surrounded by damaged cells, their behavior shifts. The activation threshold drops, and the magnitude of their response to any stimulus increases. Latremoliere and Woolf described this as peripheral sensitization: a reduction in threshold and amplification in responsiveness of nociceptors that represents a form of pain driven by nociceptor activation at the peripheral level (Latremoliere & Woolf, 2009).
This process is initially protective. An injured muscle should hurt more easily so you avoid further damage while it heals. The clinical problem arises when the nociceptive source is a trigger point, because trigger points can produce continuous low-grade irritation for weeks, months, or years without spontaneously resolving. The peripheral sensitization never turns off because the input never stops.
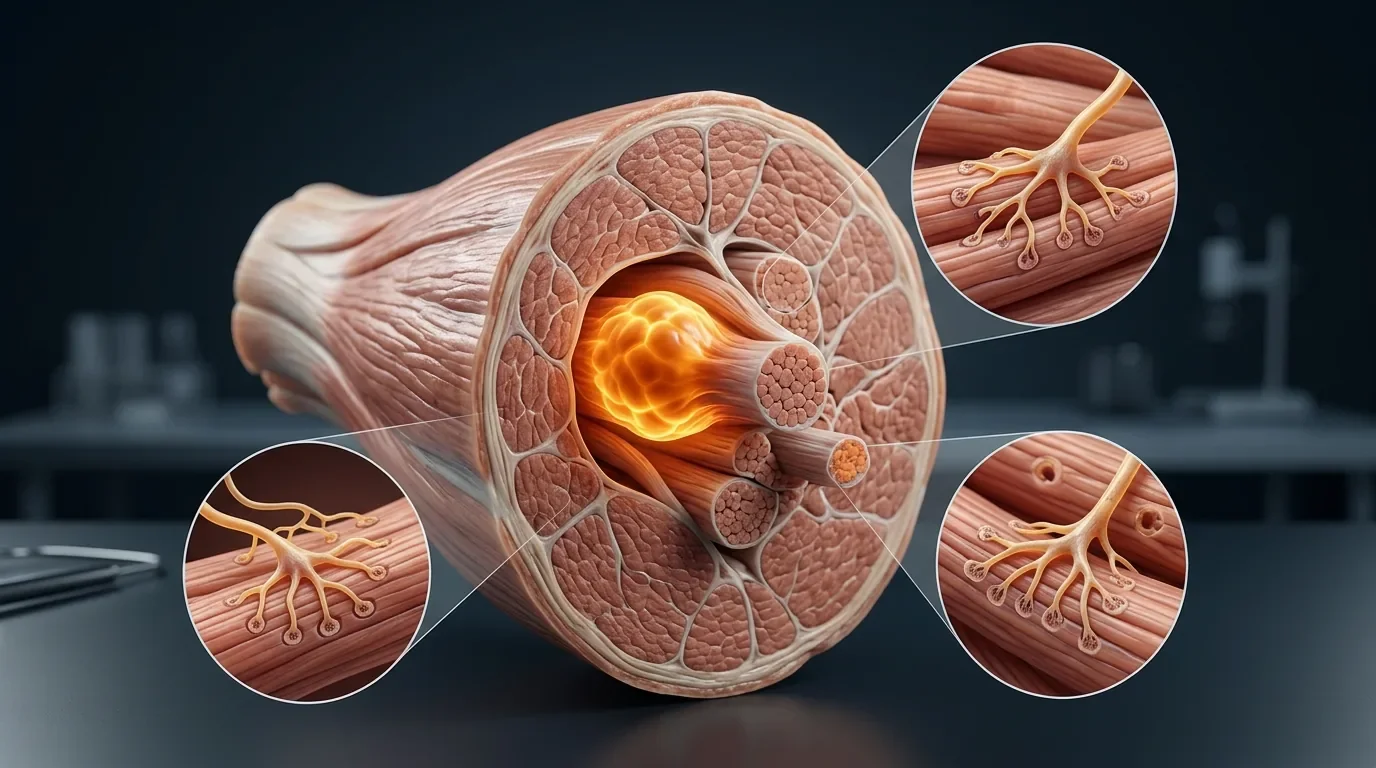
Two chemical substances are especially effective at driving this process in muscle tissue. ATP activates muscle nociceptors primarily by binding to P2X3 receptor molecules on the nerve ending membrane. Hydrogen ions, which accumulate as local pH drops (a hallmark of the trigger point environment), bind to TRPV1 and acid-sensing ion channels (ASICs). Both receptor types are channel proteins that allow sodium to flood into the neuron, generating the electrical signal the brain reads as pain (Mense, 2008).
Part 1 What Is Myofascial Pain? The Biochemistry Inside a Trigger PointThe Five-Minute Rewiring: How Muscle Injury Creates New Pain Maps
The most compelling experimental demonstration of how referred pain develops comes from a 1993 study by Hoheisel, Mense, and Simons. They isolated individual neurons in the rat spinal cord that responded exclusively to deep pressure in one specific muscle (the biceps femoris). They then injected bradykinin, a potent inflammatory pain substance, into a completely different muscle (the tibialis anterior) that was outside the neuron's receptive field.
Within five minutes, 43% of the tested neurons had developed brand-new receptive fields in deep muscle tissues they had previously ignored entirely. The nociceptive barrage from the injected muscle had unmasked dormant synaptic connections in the spinal cord, effectively recruiting these neurons to process pain from tissues they had never previously monitored.
After fifteen minutes, the changes went further: some neurons began responding to moderate, non-painful pressure in their original receptive field, a stimulus that had been well below their threshold before the experiment. In other words, a noxious stimulus in one location had both expanded the territory of pain processing and lowered the threshold for activation in existing territories (Hoheisel et al., 1993).
Turn Off the Source, Turn Off the Spread
A critical question for treatment is whether referred pain, once established, becomes independent of its source. Rubin and colleagues tested this by creating referred pain with intramuscular hypertonic saline injections and then blocking the injection site with local anesthetic. The referred pain resolved when the primary nociceptive input was silenced (Rubin et al., 2009).
This finding is directly relevant to clinical practice. It means that for trigger point referred pain, treating the source muscle should collapse the entire referred pattern. Conversely, treating only where the patient feels pain (the referral zone) is unlikely to produce lasting results because the spinal cord changes sustaining the spread depend on continuous input from the original trigger point.
Rubin's group also demonstrated that repeated nociceptive stimuli over time produced a shift: local pain intensity decreased while referred pain expanded. This progressive migration of pain from local to referred patterns with chronicity suggests that the spinal cord increasingly amplifies and redirects the signal as the condition persists, a bridge to the central sensitization mechanisms covered in Part 4 (Rubin et al., 2010).
Related Active vs. Latent Trigger Points: Types, Differences, and TreatmentHeadaches, Jaw Pain, or Arm Symptoms Nobody Can Explain?
Many patients we see have been evaluated for the wrong structure. Their headache is referred from a neck trigger point. Their arm pain comes from the scalenes, not a disc. Identifying and treating the muscular source changes everything.
Schedule NowTrigger Points as Peripheral Pain Generators
These findings position active trigger points as one of the most clinically significant peripheral pain generators for both regional and widespread musculoskeletal conditions. The local pain and tenderness at trigger points is largely driven by nociceptor sensitization from the ischemic, acidic, chemically irritated environment described in Parts 1 and 2 of this series.
Even in fibromyalgia, a condition typically characterized as a "central" pain disorder, peripheral input from muscles appears to play a sustaining role. Staud and colleagues conducted a randomized, double-blind, placebo-controlled study in which lidocaine injections into muscle tissue increased local pain thresholds and decreased remote secondary heat hyperalgesia in fibromyalgia patients. Their conclusion was that peripheral impulse input plays an important role in maintaining central sensitization in FM (Staud et al., 2009).
The Debate: Does Chronic Pain Still Need Peripheral Input?
The pain science community remains divided on whether chronic pain is primarily maintained by ongoing peripheral nociceptive signals or by central nervous system changes that have become self-sustaining. The first view holds that once pain is chronic, the original injury has healed and peripheral nociceptors contribute little to the ongoing experience. The second holds that every chronic pain state has an active nociceptor maintaining it.
The clinical evidence from trigger point treatment consistently supports the second view. Patients with years of chronic pain sometimes experience substantial relief after targeted dry needling of specific trigger points, suggesting that the peripheral driver was active all along. As one prominent researcher has argued, while central sensitization is undeniably important in pain and motor dysfunction, it is still maintained by peripheral nociceptive inputs. The practical implication for patients is that identifying and treating active trigger points remains essential even when the pain picture appears complex or widespread.
What This Means for Your Treatment
If your pain has spread, radiates, or shows up in areas where imaging finds no structural problem, it is not imaginary. It follows predictable neurological rules. Treating the peripheral source, typically one or more active trigger points, can collapse the entire referred pattern because the spinal cord changes that maintain the spread depend on ongoing input from the original site. A thorough trigger point examination by a practitioner who understands referred pain mapping is often the most efficient path to identifying why your pain behaves the way it does.
Related Trigger Points Guide: Complete Muscle Index and Referred Pain PatternsExpert Referred Pain Diagnosis at Morningside Acupuncture
At Morningside Acupuncture, we are the highest-rated acupuncture and dry needling clinic in New York City with over 500 five-star Google reviews. Our practitioners specialize in tracing referred pain to its muscular source and treating it directly. If your pain has been misdiagnosed or treatments keep targeting the wrong location, we can help.
Schedule NowReferences
- Hoheisel, U., Mense, S., Simons, D.G., & Yu, X.M. (1993). Appearance of new receptive fields in rat dorsal horn neurons following noxious stimulation of skeletal muscle: A model for referral of muscle pain? Neuroscience Letters, 153(1), 9-12. https://doi.org/10.1016/0304-3940(93)90064-r
- Latremoliere, A., & Woolf, C.J. (2009). Central sensitization: A generator of pain hypersensitivity by central neural plasticity. The Journal of Pain, 10(9), 895-926. https://doi.org/10.1016/j.jpain.2009.06.012
- Mense, S. (2008). Muscle pain: Mechanisms and clinical significance. Deutsches Arzteblatt International, 105(12), 214-219. https://doi.org/10.3238/arztebl.2008.0214
- Nijs, J., Van Houdenhove, B., & Oostendorp, R.A.B. (2010). Recognition of central sensitization in patients with musculoskeletal pain: Application of pain neurophysiology in manual therapy practice. Manual Therapy, 15(2), 135-141. https://doi.org/10.1016/j.math.2009.12.001
- Rubin, T.K., et al. (2009). Effects of intramuscular anesthesia on the expression of primary and referred pain induced by intramuscular injection of hypertonic saline. The Journal of Pain, 10(8), 829-835. https://doi.org/10.1016/j.jpain.2009.01.267
- Rubin, T.K., et al. (2010). Changes in the spatiotemporal expression of local and referred pain following repeated intramuscular injections of hypertonic saline. The Journal of Pain, 11(8), 737-745.
- Staud, R., Nagel, S., Robinson, M.E., & Price, D.D. (2009). Enhanced central pain processing of fibromyalgia patients is maintained by muscle afferent input: A randomized, double-blind, placebo-controlled study. Pain, 145(1-2), 96-104. https://doi.org/10.1016/j.pain.2009.05.020
Disclaimer: This web site is intended for educational and informational purposes only. Reading this website does not constitute providing medical advice or any professional services. This information should not be used for diagnosing or treating any health issue or disease. Those seeking medical advice should consult with a licensed physician. Seek the advice of a medical doctor or other qualified health professional for any medical condition. If you think you have a medical emergency, call 911 or go to the emergency room. No acupuncturist-patient relationship is created by reading this website or using the information. Morningside Acupuncture PLLC and its employees and contributors do not make any express or implied representations with respect to the information on this site or its use. For any legal interpretation of scope of practice in your state, consult a licensed attorney or regulatory authority.
Read more from our blog