Types of Trigger Points
Active vs Latent Trigger Points: Understanding the Key Differences
You know the sensation: a tender, tight knot in your muscle that hurts when you touch it, but does not seem to cause any spontaneous pain. Or perhaps the opposite—a painful area that, when examined, seems to have a specific point that is more tender than the surrounding tissue. These are trigger points, and understanding whether they are "active" or "latent" is the key to understanding your pain, why certain areas hurt, why other areas dysfunction without hurting, and how to design an effective treatment strategy.
The distinction between active and latent trigger points is clinically crucial but often overlooked. Both are the same underlying pathophysiology—localized regions of sustained muscle contraction with disrupted blood flow and accumulated metabolic waste. Yet they create different symptoms and have different implications for your health. An active trigger point causes spontaneous pain; a latent trigger point causes dysfunction without spontaneous pain, yet may progress to become active if untreated. Both require treatment, but the goals and approaches differ.
This article explores the science-based distinction between active and latent trigger points. We will examine how they develop, why some trigger points hurt and others do not, how latent trigger points often cause the worst functional limitations, why latent trigger points frequently progress to become active, how they are diagnosed and treated differently, and why a comprehensive treatment approach must address both types. Understanding these distinctions will help you make sense of your pain, understand your practitioner's treatment approach, and appreciate the importance of addressing trigger points before they worsen.
Whether you have one obvious painful trigger point or numerous painless areas of dysfunction, this knowledge will help you understand the underlying mechanisms and take proactive steps toward complete recovery rather than simply managing acute pain symptoms.
Key Points
- Active trigger points cause spontaneous, referred pain; latent trigger points cause dysfunction and palpable tenderness but not spontaneous pain.
- Both active and latent trigger points have the same underlying pathophysiology: sustained muscle fiber contraction, reduced blood flow, and metabolic waste accumulation.
- Latent trigger points often cause worse functional limitations than active trigger points, even though they do not hurt spontaneously.
- Latent trigger points exist in a precarious state: any stress or overuse can activate them, converting them to active trigger points.
- Active trigger points typically develop from acute trauma or sudden overload; latent trigger points typically develop from chronic overuse and repetitive strain.
- Treatment of latent trigger points is crucial for prevention: addressing them before activation saves pain and dysfunction.
- A comprehensive treatment approach must address both active and latent trigger points simultaneously, with different treatment emphases for each.
- Understanding trigger point status helps patients understand why dysfunction may persist even when pain has resolved.
Defining Active Trigger Points: Spontaneous Pain and Referred Symptoms
An active trigger point is defined clinically by one characteristic: it produces spontaneous pain. Not pain only when pressed, but pain that the patient experiences without any external stimulus. This spontaneous pain is often described as a dull, aching, ongoing sensation, though it may vary in intensity throughout the day.
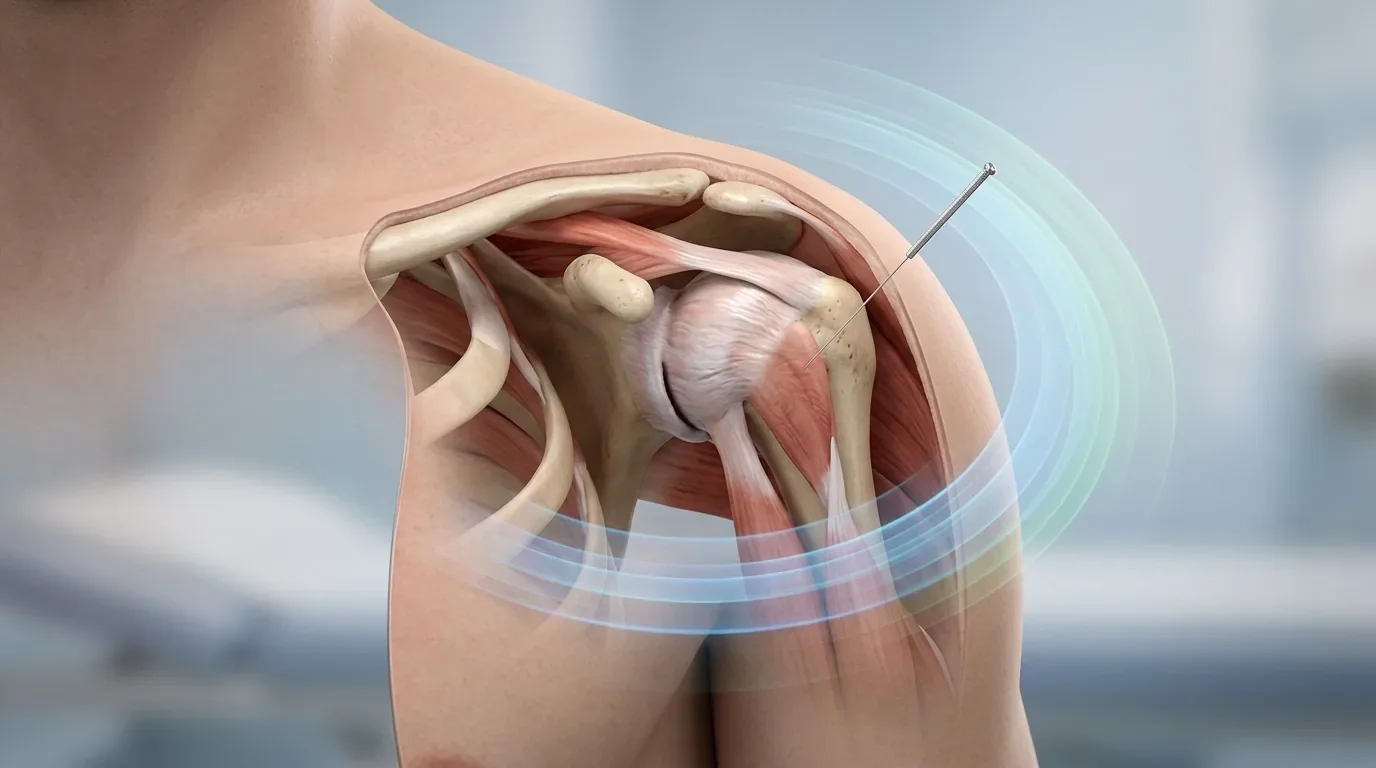
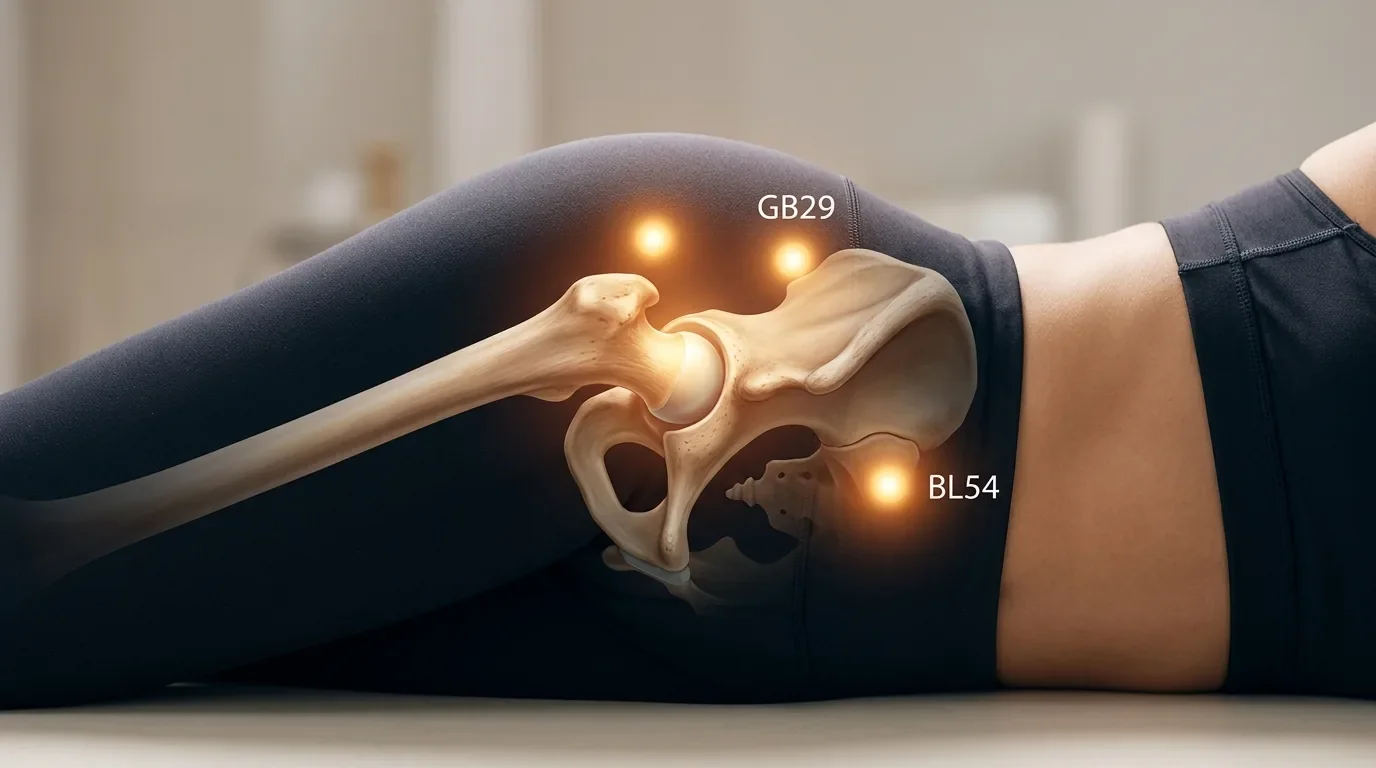
A second characteristic of active trigger points is that they produce referred pain—pain felt in an area of the body distant from the trigger point itself. For example, a trigger point in the upper trapezius muscle (upper shoulder) may refer pain down the arm; a trigger point in the gluteus medius (hip) may refer pain down the leg. The referred pain follows predictable patterns that have been mapped through decades of clinical observation. These referred pain patterns are highly recognizable to experienced practitioners and help identify which trigger point is responsible for a given pain complaint.
The spontaneous pain of an active trigger point is typically constant or near-constant, though it may fluctuate. Many patients describe good days and bad days, but even on good days, they are aware of the underlying pain. This chronic pain state often leads to secondary problems: sleep disruption (because the pain prevents deep sleep), anxiety (because constant pain is psychologically wearing), reduced activity (because movement aggravates the pain), and deconditioning (because reduced activity leads to weakness and loss of flexibility).
Active trigger points typically develop in response to acute trauma, sudden overload, or acute flare-up of a pre-existing condition. A person who suddenly lifts a heavy object incorrectly, experiences a sudden impact injury, or significantly increases activity level may develop active trigger points acutely. The pain begins suddenly or escalates from low-level to severe, and the patient seeks treatment because the pain is so obviously bothersome.
The presence of spontaneous pain makes active trigger points clinically obvious and compelling. Patients are motivated to seek treatment, and practitioners know exactly where to focus because the patient can point to the pain. However, this obviousness can be deceptive—active trigger points often develop superimposed on a foundation of latent trigger points that have been present for months or years. If only the active trigger points are treated and the latent ones are ignored, pain relief may be temporary because the underlying predisposing condition remains.
Defining Latent Trigger Points: Dysfunction Without Spontaneous Pain
A latent trigger point, by contrast, does not produce spontaneous pain. A person with latent trigger points may experience no pain while at rest and no pain with normal activity. They feel well. Yet if a practitioner palpates (manually examines) the muscle tissue, they will find a tender, tight nodule. When pressure is applied to this point, it produces local pain (tenderness at the point being pressed) or may produce referred pain if that trigger point's typical referred pain pattern is elicited.
The critical distinction is this: the pain is produced only by external pressure; it is not present spontaneously. Many patients are surprised when a practitioner identifies a tender point they were completely unaware of. "I did not even know that was there," they say—which is the defining characteristic of a latent trigger point.
Latent trigger points are defined not by pain but by dysfunction. The muscle containing a latent trigger point typically exhibits:
- Weakness: The muscle is weaker than its contralateral (opposite side) counterpart or its baseline strength.
- Reduced flexibility: The muscle cannot stretch as far as normal.
- Reduced endurance: The muscle fatigues more quickly with sustained activity.
- Stiffness: The muscle feels tight, even when resting.
- Movement dysfunction: The person may demonstrate compensatory movement patterns because the affected muscle is not functioning optimally.
These functional limitations may be subtle. A person with latent trigger points in their hip muscles may not notice obvious weakness, but a physical therapist testing hip strength will find measurable deficit. A person with latent trigger points in their shoulder muscles may not notice obvious limitation in range of motion, but overhead activities may feel stiff or awkward.
Latent trigger points typically develop gradually, through chronic overuse or repetitive strain. A person who sits at a desk for eight hours daily will gradually develop latent trigger points in their hip flexors, upper trapezius, and neck muscles. A person who repetitively performs overhead activity (as in tennis or painting) may develop latent trigger points in their rotator cuff muscles. These develop insidiously, over weeks or months, so gradually that the person may not remember when the dysfunction started.
The Shared Pathophysiology: Why Both Types Are Actually Trigger Points
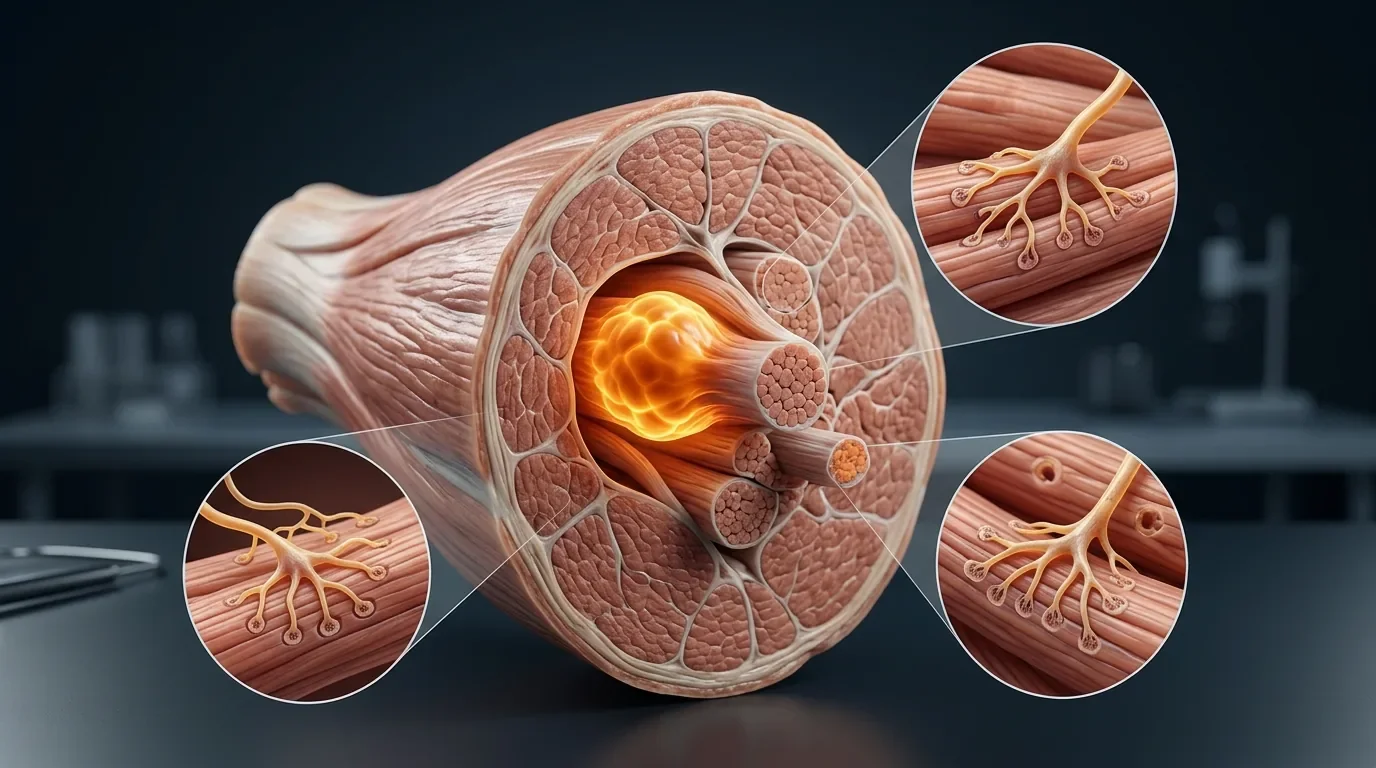
Despite their different presentations, active and latent trigger points are characterized by the same underlying pathophysiology. Both are regions of sustained muscle fiber contraction—sometimes called "taut bands" because the contracted muscle fibers form a tight band within the larger muscle.
Within both types of trigger points, the following changes are present:
Sustained Muscle Contraction: Individual muscle fibers remain in a state of partial contraction even at rest. This is not voluntary—the person cannot consciously relax these fibers. Rather, it is an involuntary sustained contraction, as if the "off switch" for those fibers is stuck.
Reduced Blood Flow: The sustained contraction compresses local blood vessels, reducing the flow of oxygen-rich blood to the muscle fibers. This compression is mechanical and direct—the tight muscle tissue physically squeezes the capillaries running through it.
Hypoxia (Low Oxygen): The reduced blood flow leads to a state of low oxygen (hypoxia) in the affected tissue. Muscle fibers are aerobic organisms—they prefer to burn oxygen for energy. When oxygen is limited, they must shift to anaerobic metabolism, which is less efficient and produces more metabolic waste.
Accumulation of Metabolic Waste: The anaerobic metabolism produces lactic acid, hydrogen ions, and other metabolic byproducts that accumulate in the hypoxic tissue. These molecules are irritating to the surrounding tissue and the nerve endings in the area. This chemical irritation is a major driver of trigger point tenderness and pain.
Altered Neurological Signaling: The irritated local tissue triggers ongoing activity in nociceptors (pain-sensing nerve endings) and mechanoreceptors (sensory organs detecting pressure and stretch). These receptors send continuous signals to the spinal cord and brain, informing the nervous system that something is wrong in this region. The nervous system responds by maintaining muscle tension as a protective mechanism—further perpetuating the problem.
This vicious cycle—contraction, reduced blood flow, hypoxia, waste accumulation, nerve irritation, protective guarding—is the same in active and latent trigger points. The only difference is in the amplitude of the cycle and in how the nervous system is interpreting the signals.
In an active trigger point, the cycle is intense enough that the nervous system is receiving strong pain signals even at rest. The persistent irritation has reached a level where the brain perceives pain spontaneously.
In a latent trigger point, the cycle exists but is of lower amplitude. The local irritation is present and detectable on palpation, but the nervous system is not interpreting the signals as threatening enough to generate spontaneous pain. The dysfunction is real, but the pain perception has not yet escalated.
From Latent to Active: How Trigger Points Worsen Over Time
The relationship between latent and active trigger points is not random or arbitrary. Rather, latent trigger points exist in a precarious state. Under the right (or wrong) circumstances, they readily convert to active trigger points. This progression is one of the most important concepts in understanding trigger point pathophysiology.
What causes latent trigger points to activate? Several factors increase the risk:
Acute Overload: A person with latent trigger points in their lower back participates in heavy lifting. The acute overload on muscles already compromised by latent trigger points overwhelms them. The sustained contraction intensifies, the local irritation becomes severe enough to generate spontaneous pain, and the latent trigger point becomes active.
Repetitive Activity Beyond the Muscle's Capacity: A person whose shoulder muscles contain latent trigger points begins a new job requiring repetitive overhead motion. The repetitive demand accumulates stress on an already-compromised muscle. The sustained contraction intensifies, and what was latent becomes active.
Inadequate Recovery: A person with latent trigger points in their neck takes a job with increased stress and poor sleep quality. The muscle is not recovering between work sessions. Fatigue accumulates, the sustained contraction persists even during supposed rest, and the trigger point transitions to active.
Loss of Stabilization: A person with latent trigger points in their hip muscles suffers a knee injury that reduces their stability. The hip muscles, now required to work harder to stabilize an unstable structure, become overwhelmed. The sustained contraction intensifies, and activation occurs.
Emotional Stress and Sympathetic Activation: Emotional stress triggers sympathetic nervous system activation and muscle tension. A person with latent trigger points experiences significant emotional stress. Their baseline muscle tension increases, further elevating the tension in muscles containing latent trigger points. This elevated tension pushes the already-stressed muscles over the threshold from latent to active.
The key insight is this: latent trigger points represent a state of compensated dysfunction. The muscle is not working normally, but the person is managing. The system is stable but fragile. Any additional stress can destabilize it. This is why people sometimes report that their pain began suddenly: "I was fine, and then I did one more thing and suddenly I was in pain." The reality is that the groundwork had been laid by months or years of latent trigger point development. The acute event was simply the final straw.
Conversely, if latent trigger points are treated before they activate, the risk of progression to active trigger points is significantly reduced. A person who addresses latent trigger points proactively through dry needling, stretching, and activity modification may prevent the acute pain crisis entirely. This is a major reason why practitioners recommend treating latent trigger points even when the patient does not have spontaneous pain—preventing activation is easier and less disruptive than treating active trigger points.
Clinical Diagnosis: How Practitioners Differentiate Active and Latent Trigger Points
Correctly identifying whether a trigger point is active or latent is crucial for treatment planning. The diagnosis is primarily clinical, based on the patient's report of symptoms and the practitioner's physical examination findings.
Patient History and Symptoms: The practitioner asks detailed questions about pain: Do you have pain right now? Is the pain constant or intermittent? Does the pain occur spontaneously or only with activity? Does the pain occur in one location or in multiple areas (suggesting referred pain)? The presence of spontaneous pain localized to a specific region or with a recognized referred pain pattern strongly suggests an active trigger point in a specific muscle.
Palpation (Physical Examination): The practitioner systematically palpates muscles, feeling for taut bands and tender points. When a tender point is identified, the practitioner applies pressure. If the patient experiences a spontaneous pain that they recognize as similar to their baseline pain complaint—especially if it reproduces a familiar referred pain pattern—this confirms an active trigger point. If pressure produces only local tenderness, with no spontaneous pain and no referred pain, the trigger point is likely latent.
Functional Assessment: The practitioner assesses muscle strength, flexibility, and endurance. A muscle with an active trigger point is typically weak and stiff. A muscle with only latent trigger points may also demonstrate weakness and stiffness, but the functional deficit often exceeds what would be expected from pain alone. This discordance—significant functional limitation despite minimal or no pain—is characteristic of latent trigger points.
The distinction is not always crystal clear. Some trigger points may be partially active—producing some spontaneous pain but not reaching the full intensity that would warrant diagnosis as truly active. A skilled practitioner learns to recognize these gradations and to use the information to guide treatment.
The Clinical Significance of Latent Trigger Points: Why "No Pain" Does Not Mean "No Problem"
One of the most important clinical insights is that latent trigger points, despite their lack of spontaneous pain, often cause worse functional limitations than active trigger points. This seems counterintuitive—how can something that does not hurt create worse dysfunction than something that does hurt?
The answer lies in the nature of dysfunction. An active trigger point causes pain, which naturally limits activity. A person with severe active trigger point pain in their shoulder will limit shoulder movement because the pain prevents it. The body is actually protecting itself—the pain serves a purpose, preventing movement that might worsen the injury.
A latent trigger point, producing no spontaneous pain, offers no such protective limitation. The person feels fine. They move normally, exercise normally, work normally. Yet the muscle is dysfunctional—weak, tight, fatiguing quickly. This permits activities that might actually be harmful, given the muscle's compromised state. A person with latent trigger points in their rotator cuff feels fine and continues throwing (as a baseball player) or serving (as a tennis player) at full intensity. The compromised muscles cannot handle the load, and damage accumulates. By the time the trigger point activates and pain develops, significant tissue damage may have already occurred.
Additionally, latent trigger points create compensation patterns. When one muscle is dysfunctional, other muscles increase their activity to compensate. These compensatory muscles are not designed for the increased load and themselves develop latent trigger points. A person may develop a cascade of trigger points starting with one latent trigger point, as the entire kinetic chain becomes involved in compensation.
For example, a person with a latent trigger point in their gluteus medius (hip muscle) continues running at their normal pace. The dysfunctional gluteus medius cannot stabilize the hip properly, so the hip adductors and lower back muscles work harder to compensate. These muscles develop their own latent trigger points. The person still feels fine and continues running, but their entire lower body is becoming progressively more dysfunctional. When pain finally develops, it may not be localized to the original latent trigger point but distributed across multiple muscles and multiple referred pain patterns.
This is why practitioners often recommend comprehensive assessment and treatment even for patients without significant pain. A patient coming in with acute shoulder pain may actually have a network of latent trigger points throughout their shoulder, neck, and upper back that have been present for months or years. Treating only the obviously active painful points leaves the latent network intact, and pain is likely to recur when activity increases again.
Treatment Approaches: Active Versus Latent Trigger Point Management
Although active and latent trigger points have the same underlying pathophysiology, their treatment approaches emphasize different goals, and the treatment intensity and urgency typically differ.
Active Trigger Point Treatment: The primary goal is rapid pain relief and restoration of basic function. Treatment is typically more intensive—patients are usually seen 1-2 times weekly during the acute phase. Dry needling or other treatments are performed with the goal of eliciting multiple local twitch responses and thoroughly disrupting the sustained contraction cycle. The frequency of treatment is justified because the pain is severe and limiting, and rapid relief improves the patient's quality of life and allows them to participate in rehabilitation.
Active trigger points respond well to aggressive treatment because the muscles are already highly irritable and reactive. A single effective needle contact typically produces a strong local twitch response and often immediate pain relief. The goal is to break the acute cycle and reduce spontaneous pain to a level that allows normal movement and sleep.
Treatment of active trigger points focuses on achieving pain relief quickly, after which the focus shifts to addressing underlying dysfunction and preventing recurrence.
Latent Trigger Point Treatment: The primary goal is to normalize muscle function and prevent activation to active. Treatment is typically less intensive—patients may be seen monthly or every 6-8 weeks for preventive treatment of latent trigger points. However, if a patient has numerous latent trigger points and significant functional limitation, more frequent initial treatment may be warranted.
Treatment of latent trigger points may be less "aggressive" in that the goal is not maximum local twitch response frequency (since the muscles are not in acute pain and not requiring pain relief) but rather consistent normalization of muscle fiber function and restoration of normal blood flow and metabolic function.
Treatment of latent trigger points emphasizes prevention and long-term functional optimization. The goal is to maintain the muscle in a functional state and prevent progression to active trigger points through ongoing management. This often includes patient education about activity modification, stretching, ergonomics, and other lifestyle factors that prevent latent trigger points from accumulating or worsening.
Combined Approach: In reality, most patients have both active and latent trigger points. The most effective treatment approach addresses both. Initial focus is on the active trigger points to achieve pain relief (because pain is the chief complaint and often the most limiting factor). But simultaneously, latent trigger points are identified and addressed to prevent future activation and to address the underlying dysfunction. As the acute pain resolves, the focus shifts increasingly toward latent trigger point management and functional rehabilitation.
Rehabilitation and Prevention: The Long-Term Management of Trigger Points
Treatment of trigger points—both active and latent—does not end with dry needling or other manual therapy. In fact, the manual therapy may be the quickest part of treatment. The longer-term challenge is rehabilitation and prevention of recurrence.
Rehabilitation After Active Trigger Points: Once acute pain from active trigger points is controlled, rehabilitation focuses on restoring strength, flexibility, and endurance to the affected muscles. The patient performs targeted stretching to regain full range of motion and exercises to rebuild strength. This rehabilitation is crucial because it addresses the deconditioning and weakness that developed while pain was limiting activity. Without rehabilitation, patients are at high risk of pain recurrence because the muscle remains weak and dysfunctional.
Prevention of Latent Trigger Point Activation: For latent trigger points, prevention is key. Once identified and treated, latent trigger points can be prevented from progressing to active through:
- Activity Modification: The patient learns to recognize activities that stress vulnerable muscles and modifies them. A person with latent trigger points in their neck learns proper desk ergonomics and takes regular breaks from screen time.
- Stretching and Mobility Work: Regular stretching maintains flexibility and reduces the baseline tension in muscles containing latent trigger points.
- Strengthening: Targeted strengthening of weak muscles improves their capacity to handle normal demands and reduces the risk of overload.
- Stress Management: Since emotional stress elevates muscle tension, stress management techniques (meditation, exercise, adequate sleep) reduce the risk of latent trigger points activating.
- Periodic Maintenance Treatment: Many patients benefit from periodic (monthly or every 6-8 weeks) dry needling or other treatment to maintain latent trigger points in a normalized state and prevent accumulation of new latent trigger points.
This long-term management approach is often more important than the acute treatment itself. A person who receives excellent dry needling treatment but does not engage in rehabilitation and prevention often develops recurrent active trigger points. A person who receives adequate treatment and actively participates in prevention strategies often experiences sustained relief and functional improvement.
Why Pain Relief Without Addressing Dysfunction Is Incomplete
A common pattern in pain management is that pain is treated but underlying dysfunction is ignored. A patient experiences severe pain from active trigger points, receives treatment, the pain goes away, and they feel they are cured. But the latent trigger points that preceded the acute episode are still present. The muscle is still weak. The movement patterns are still dysfunctional.
This incomplete treatment is why many patients experience pain recurrence. The underlying problem was never addressed. Any subsequent stress that activates the latent trigger points will recreate the pain.
A complete approach to trigger point management requires understanding that:
- Pain is the tip of the iceberg. The pain you feel represents the acute manifestation of a dysfunction that has been developing for months or years.
- Treating pain without addressing dysfunction is temporary. Pain relief is wonderful and important, but lasting recovery requires addressing the muscle weakness, tightness, and poor movement patterns that allowed the problem to develop.
- Latent trigger points are your warning sign. The presence of latent trigger points indicates that certain muscles are not functioning well and are at risk of further problems. Addressing them now prevents future acute episodes.
- Prevention is superior to treatment. Preventing active trigger points from developing is easier, cheaper, and less disruptive than treating them once they occur.
This is why a skilled practitioner does not simply treat the obviously painful trigger points and dismiss the patient. They conduct a thorough assessment, identify latent trigger points, explain their significance, and develop a comprehensive management plan that addresses both active and latent trigger points and includes rehabilitation and prevention strategies.
Whether you have obvious acute pain or subtle functional limitation, we can help. Our comprehensive assessment identifies both active and latent trigger points and develops a treatment plan for complete recovery.
Frequently Asked Questions
Can latent trigger points eventually become active?
Yes, absolutely. Latent trigger points exist in a precarious state and can transition to active trigger points when stressed. Acute overload, repetitive activity, inadequate recovery, or emotional stress can activate latent trigger points. This is why treating latent trigger points prophylactically—before they activate—is so important. Prevention is far easier than treatment of acute pain.
If I have latent trigger points but no pain, do I really need treatment?
Yes. Even without spontaneous pain, latent trigger points cause weakness, reduced flexibility, and reduced endurance. More importantly, they increase your risk of developing acute pain with any additional stress. Treating latent trigger points now prevents future pain episodes and improves your functional capacity. It is preventive medicine.
Can a muscle have both active and latent trigger points?
Absolutely. A muscle commonly has one prominent active trigger point (causing spontaneous pain) and multiple latent trigger points (causing dysfunction without spontaneous pain). This is why comprehensive treatment must address the entire muscle, not just the obviously painful area.
How can I tell if a tender point in my muscle is an active or latent trigger point?
The key distinction is whether you experience spontaneous pain. If a tender point causes pain only when pressed but you have no spontaneous pain, it is likely latent. If you have ongoing pain that you recognize as your baseline pain problem, and palpation produces that same pain, it is likely active. Your practitioner can make the definitive determination through careful examination.
If I treat only the active trigger point and ignore latent ones, will my pain come back?
Quite possibly, yes. If latent trigger points are not addressed, they may activate with subsequent stress or activity, recreating your pain problem. A comprehensive approach that addresses both active and latent trigger points gives you the best chance of lasting recovery and prevention of recurrence.
How often should I get treated for latent trigger points?
This varies based on your activity level, stress level, and how many latent trigger points you have. Some patients benefit from monthly maintenance treatment; others do well with treatment every 6-8 weeks. Your practitioner will help you determine the optimal frequency based on your specific situation and goals.
Can stretching and exercise address latent trigger points, or do I need professional treatment?
Stretching and exercise are crucial for preventing latent trigger points from activating and for maintaining muscle function long-term. However, they alone typically cannot fully resolve latent trigger points. Professional treatment (such as dry needling) combined with stretching and exercise is most effective. The professional treatment helps reset the muscle fibers and restore blood flow; the stretching and exercise help maintain the improvements and prevent recurrence.
References
Money, S. (2017). Pathophysiology of Trigger Points in Myofascial Pain Syndrome. Journal of Pain & Palliative Care Pharmacotherapy, 31(2), 158-159. https://pubmed.ncbi.nlm.nih.gov/28379050/
Lam, C., Francio, V. T., Gustafson, K., Carroll, M., York, A., & Chadwick, A. L. (2024). Myofascial pain - A major player in musculoskeletal pain. Best Practice & Research Clinical Rheumatology, 38(1), 101944. https://pubmed.ncbi.nlm.nih.gov/38644073/
Lew, J., Kim, J., & Nair, P. (2021). Comparison of dry needling and trigger point manual therapy in patients with neck and upper back myofascial pain syndrome: a systematic review and meta-analysis. Journal of Manual & Manipulative Therapy, 29(3), 136-146. https://pubmed.ncbi.nlm.nih.gov/32962567/
Gattie, E., Cleland, J. A., & Snodgrass, S. (2017). The Effectiveness of Trigger Point Dry Needling for Musculoskeletal Conditions by Physical Therapists: A Systematic Review and Meta-analysis. Journal of Orthopaedic & Sports Physical Therapy, 47(3), 133-149. https://pubmed.ncbi.nlm.nih.gov/28158962/
Dach, F., & Ferreira, K. S. (2023). Treating myofascial pain with dry needling: a systematic review for the best evidence-based practices in low back pain. Arquivos de Neuro-Psiquiatria, 81(12), 1169-1178. https://pubmed.ncbi.nlm.nih.gov/38157883/
Navarro-Santana, M. J., Sanchez-Infante, J., Fernandez-de-Las-Penas, C., Cleland, J. A., Martin-Casas, P., & Plaza-Manzano, G. (2020). Effectiveness of Dry Needling for Myofascial Trigger Points Associated with Neck Pain Symptoms: An Updated Systematic Review and Meta-Analysis. Journal of Clinical Medicine, 9(10), 3300. https://pubmed.ncbi.nlm.nih.gov/33066556/
Ma, X., Qiao, Y., Wang, J., Xu, A., & Rong, J. (2024). Therapeutic Effects of Dry Needling on Lateral Epicondylitis: An Updated Systematic Review and Meta-analysis. Archives of Physical Medicine and Rehabilitation, 105(11), 2184-2197. https://pubmed.ncbi.nlm.nih.gov/38484834/
Complete Recovery Requires Comprehensive Trigger Point Management
Understanding the distinction between active and latent trigger points is the key to understanding your pain, your dysfunction, and your path to recovery. Active trigger points are obvious—they demand attention through pain. Latent trigger points are subtle—they operate behind the scenes, causing weakness and dysfunction that you may not notice until they activate and create acute pain.
Complete recovery requires addressing both. It requires treating the acute pain of active trigger points so you can function and sleep. It requires identifying and treating latent trigger points to prevent future acute episodes and to restore full functional capacity. And it requires engagement in rehabilitation and prevention to maintain your improvements long-term.
At Morningside Acupuncture, we provide this comprehensive approach. We do not simply treat your pain; we assess your entire muscular system, identify all trigger points, and develop a treatment plan that addresses both active and latent trigger points. This comprehensive approach ensures not just pain relief but lasting functional improvement. Contact us today to begin your journey toward complete recovery.
Disclaimer: This content is for educational and informational purposes only and does not constitute medical advice. Always consult with a qualified healthcare provider for diagnosis and treatment of any medical condition.
Disclaimer: This web site is intended for educational and informational purposes only. Reading this website does not constitute providing medical advice or any professional services. This information should not be used for diagnosing or treating any health issue or disease. Those seeking medical advice should consult with a licensed physician. Seek the advice of a medical doctor or other qualified health professional for any medical condition. If you think you have a medical emergency, call 911 or go to the emergency room. No acupuncturist-patient relationship is created by reading this website or using the information. Morningside Acupuncture PLLC and its employees and contributors do not make any express or implied representations with respect to the information on this site or its use. For any legal interpretation of scope of practice in your state, consult a licensed attorney or regulatory authority.
Read more from our blog