What is Myofascial Pain?
The Science Behind Muscle Pain, Trigger Points, and Why It Remains Overlooked
Myofascial pain syndrome is one of the most common sources of chronic musculoskeletal pain, yet no medical specialty claims skeletal muscle as its primary organ. Here is what the research tells us about why muscles hurt, what happens inside a trigger point, and why this matters for your treatment.
- Myofascial pain syndrome (MPS) is caused by trigger points: hyperirritable spots in taut bands of skeletal muscle that typically produce referred pain.
- Studies estimate that 42% to 47% of pain clinic patients present with myofascial pain, yet it remains widely underdiagnosed because no medical specialty "owns" skeletal muscle (Simons, 2007).
- The integrated trigger point hypothesis describes a self-sustaining cycle of motor endplate dysfunction, localized ischemia, acidic pH, nociceptor sensitization, and sarcomere contraction.
- Microdialysis research has identified significantly elevated levels of inflammatory and pain-related biochemicals (substance P, CGRP, norepinephrine, serotonin, TNF-alpha, interleukins) in the immediate environment of active trigger points (Shah et al., 2005; Shah et al., 2008).
- Dry needling may modulate these biochemicals in a dosage-dependent manner, reducing substances associated with pain, inflammation, and tissue hypoxia (Hsieh et al., 2012).
- Multiple contraction types, from sustained low-level desk work to eccentric exercise, can contribute to trigger point development through localized energy crisis and calcium dysregulation.
Is Myofascial Pain the Source of Your Chronic Muscle Pain?
Trigger points are one of the most common and most overlooked causes of persistent pain. At Morningside Acupuncture, we specialize in identifying and treating myofascial trigger points using dry needling and targeted acupuncture. Schedule your evaluation today.
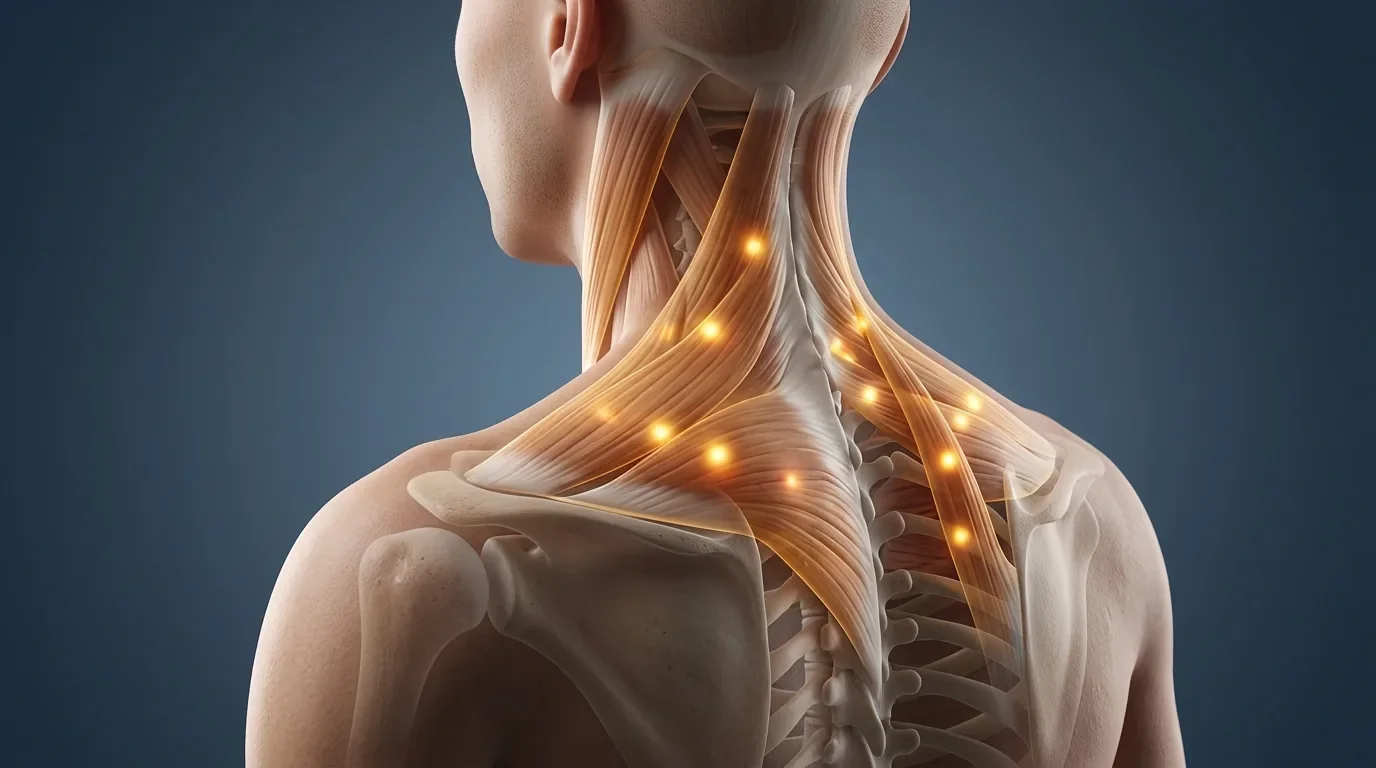
Schedule NowIf you have ever had a deep, aching knot in your neck, shoulder, or back that seemed to send pain somewhere else entirely, you have likely experienced myofascial pain. It is remarkably common, yet it remains one of the most underrecognized conditions in modern medicine.
The term "myofascial" combines myo (muscle) and fascia (the connective tissue that surrounds muscle fibers). Myofascial pain syndrome (MPS) refers to a chronic pain condition driven by myofascial trigger points: small, hyperirritable spots located within taut bands of skeletal muscle. These trigger points characteristically produce referred pain, meaning the pain you feel may show up in a location that is distant from the actual source of the problem.
As the late Dr. David Simons wrote in his landmark editorial, skeletal muscle is effectively an "orphan organ" because no medical specialty claims it as its primary focus (Simons, 2007). Orthopedics focuses on bones and joints. Neurology focuses on nerves. Rheumatology focuses on autoimmune and connective tissue diseases. Skeletal muscle, the single largest organ system in the body by mass, falls through the cracks. The result is that MPS is frequently overlooked, misdiagnosed as joint pathology, or attributed entirely to structural findings on imaging that may not be the true source of a patient's pain.
Related Trigger Points Guide: Complete Muscle Index and Treatment OverviewHow Common Is Myofascial Pain?
The true incidence of MPS is difficult to pin down, in large part because diagnostic criteria have historically varied across studies and specialties. However, survey data from pain management providers paints a consistent picture: myofascial pain is extremely prevalent. In studies surveying pain clinic populations, 42% to 47% of patients were identified as having a myofascial pain component (Fleckenstein et al., 2010; Harden et al., 2000).
Pain medicine specialists tend to value myofascial pain as a diagnostic entity more than physicians in other specialties. A cross-sectional nationwide survey found a notable discrepancy between how frequently clinicians encounter myofascial pain and how often they feel adequately trained to treat it (Fleckenstein et al., 2010). This gap extends into physical therapy education as well: fewer than 50% of PT program faculty surveyed were aware of the Institute of Medicine report on pain or the IASP guidelines for pain education, and only 61% believed their students received adequate pain management training (Hoeger Bement & Sluka, 2014).
Myofascial trigger points are not limited to adults. Research has documented trigger points and increased deep tissue mechanical sensitivity in children, suggesting that the physiological substrate for trigger point development may be present from early life (Kao et al., 2007; Han et al., 2012).
The Integrated Trigger Point Hypothesis: What Happens Inside a Trigger Point
The most widely accepted model for explaining the pathophysiology of myofascial trigger points is the Integrated Trigger Point Hypothesis, originally proposed by Simons and subsequently expanded by Gerwin, Dommerholt, and Shah (Gerwin et al., 2004). This hypothesis describes a self-perpetuating cycle that begins with muscle overload and cascades through several interconnected mechanisms.
Here is how the cycle works, in plain terms:
Muscle overload, whether from acute trauma, repetitive activity, or sustained low-level contraction, leads to localized ischemia (reduced blood supply) and hypoxia (oxygen deprivation) in the affected tissue. Reduced oxygen availability causes the local pH to drop, creating an acidic environment. This pH shift activates acid-sensing ion channels (ASIC1 and ASIC3) on nearby muscle nociceptors, which may produce mechanical hyperalgesia: increased sensitivity to pressure and touch (Sluka et al., 2007).
The acidic environment also inhibits acetylcholinesterase (AChE), the enzyme responsible for breaking down acetylcholine (ACh) at the motor endplate. With AChE inhibited, ACh accumulates at the neuromuscular junction, and nicotinic ACh receptors become upregulated. The result is increased miniature endplate potential (MEPP) frequency, sustained actin-myosin interaction, and persistent sarcomere contraction, all without a voluntary command from the nervous system.
This sustained contraction compresses local blood vessels, worsening the ischemia, which in turn deepens the energy crisis. Meanwhile, nociceptive substances accumulate in the local tissue, sensitizing peripheral nerve endings and feeding into the cycle of pain. The taut band and palpable nodule that clinicians identify during examination represent this contracted, energy-depleted, chemically irritated segment of muscle fiber.
| Step | What Happens (Science) | What It Means (Plain English) |
|---|---|---|
| 1. Muscle Overload | Acute, repetitive, or sustained contraction exceeds local metabolic capacity | You overwork, overstretch, or hold a muscle in one position for too long |
| 2. Ischemia & Hypoxia | Localized blood flow is impaired; oxygen delivery drops | The muscle area stops getting enough blood and oxygen |
| 3. pH Drops | Increased acidity activates ASIC1/ASIC3 nociceptors; TRPV1, TRPV4, TRPC4, TRPC5 channels may also respond | The tissue becomes acidic, which switches on pain receptors |
| 4. AChE Inhibition | Low pH suppresses the enzyme that clears acetylcholine from the motor endplate | The chemical signal telling the muscle to contract stops being cleaned up |
| 5. ACh Accumulation | Excessive ACh at the neuromuscular junction with upregulated nAChR receptors | "Contract" signals pile up at the nerve-muscle junction |
| 6. Sustained Sarcomere Contraction | Increased MEPP frequency drives persistent actin-myosin cross-bridge cycling | The muscle fibers lock into a contracted state without you telling them to |
| 7. Taut Band / Trigger Point | Palpable nodule within a band of contracted sarcomeres; local twitch response possible | You feel a "knot" that may twitch when pressed |
| 8. Pain & Tenderness | Referred pain, peripheral and central sensitization, CGRP and substance P release | Pain spreads beyond the knot; the area becomes more and more sensitive over time |
The Biochemical Evidence: What Microdialysis Reveals
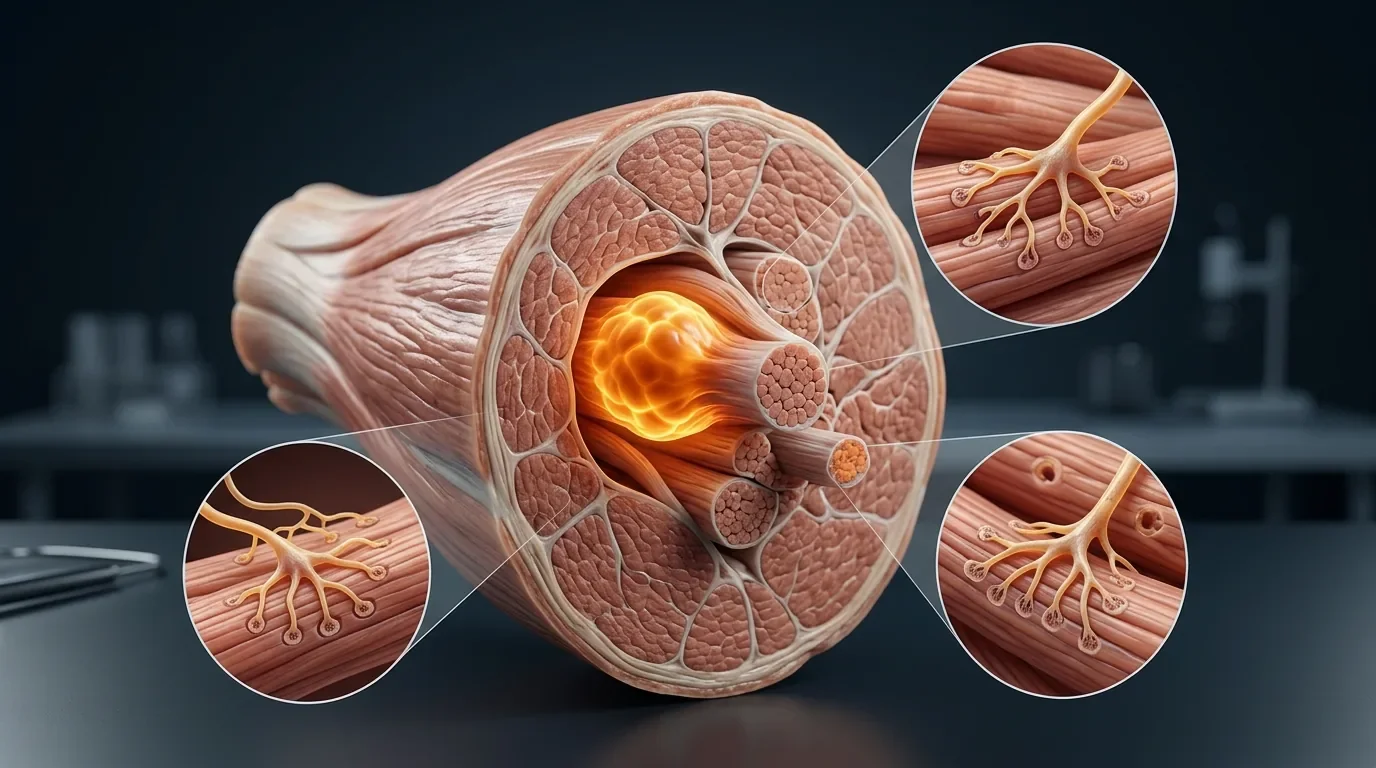
One of the most compelling lines of evidence supporting the integrated hypothesis comes from microdialysis research conducted by Shah and colleagues at the National Institutes of Health. Microdialysis is an in vivo technique that allows researchers to sample the biochemical environment of living muscle tissue by inserting a tiny probe (0.3 mm) directly into the interstitium, the fluid-filled space surrounding muscle fibers where nociceptor free nerve endings reside (Shah et al., 2005).
Using this technique, Shah's team demonstrated that the local biochemical milieu of active myofascial trigger points is dramatically different from normal muscle tissue. The pH at active trigger point sites was significantly lower (more acidic) than at non-trigger-point sites. In animal models, intracellular pH dropped from 7.0 to 6.6 during four hours of ischemia, a shift sufficient to fully activate nociceptive ASIC3 channels in nearby neurons (Hagberg, 1985).
Beyond pH, microdialysis revealed elevated concentrations of multiple pain- and inflammation-related substances at active trigger point sites, including in regions remote from (but segmentally related to) the trigger point itself (Shah et al., 2008).
| Substance | Role in the Body | Why It Matters for Pain |
|---|---|---|
| CGRP (Calcitonin Gene-Related Peptide) | Neuropeptide involved in vasodilation and neurogenic inflammation | Contributes to local swelling, increased blood flow, and pain signaling |
| Substance P | Neuropeptide that transmits pain signals to the spinal cord | Amplifies pain perception and promotes inflammatory responses |
| Norepinephrine | Catecholamine involved in sympathetic nervous system activation | May increase ACh release at the motor endplate, worsening the contraction cycle |
| Serotonin (5-HT) | Neurotransmitter with both algesic (pain-producing) and sensitization effects | Can directly activate and sensitize muscle nociceptors |
| TNF-alpha | Pro-inflammatory cytokine | Drives local inflammation and tissue damage |
| Interleukins (IL-1, IL-6, IL-8) | Pro-inflammatory cytokines | Promote ongoing inflammatory signaling and nociceptor sensitization |
| Hydrogen ions (H+) | Marker of tissue acidity | Activate acid-sensing ion channels on muscle pain receptors |
This body of work provides direct biochemical evidence that trigger points are not simply "muscle tension." They represent measurable, localized biochemical environments characterized by acidosis, elevated inflammatory mediators, and nociceptive sensitization.
Endplate Noise: Electrical Evidence of Trigger Point Dysfunction
Beyond biochemistry, electrophysiological studies have provided additional evidence for the motor endplate dysfunction described in the integrated hypothesis. Spontaneous electrical activity (SEA), also called endplate noise, has been recorded at trigger point sites using needle EMG.
Kuan and colleagues found that endplate noise was significantly more prevalent (P < 0.01) in active trigger points compared to latent trigger points. Critically, both pain intensity and pressure pain threshold were highly correlated with the prevalence of endplate noise in the trigger point region, with correlation coefficients of r = 0.742 and r = -0.716 respectively (Kuan et al., 2007). This means that the more electrically active the trigger point, the more painful it tends to be.
Interestingly, Hong and Yu (1998) demonstrated that cutting the spinal cord or peripheral nerve in animal models did not eliminate this spontaneous electrical activity, which argues that at least some component of trigger point activity is maintained at the local tissue level rather than being entirely centrally driven.
Studies of neuromuscular jitter (fluctuations in the timing of endplate potentials) have also shown that patients with myofascial trigger points demonstrate significantly increased jitter compared to healthy controls. A positive correlation between jitter and duration of myofascial pain supports the possibility of progressive neuronal changes in chronic cases (Chang et al., 2008; 2011).
What Causes Trigger Points?
There is general agreement that any form of muscle overuse or direct trauma can contribute to trigger point development (Bron & Dommerholt, 2012). The specific pathways are more varied than most patients expect. Trigger points can form from sustained low-level activity (desk work, computer use), repetitive movements (typing, assembly work), eccentric loading (downhill running, lowering weights), high-intensity concentric efforts (heavy lifting, sprinting), psychological stress (through sympathetic nervous system activation), and even visceral organ pathology (through referred pain in segmentally related muscles). In each case, the downstream result is a localized energy crisis in the affected muscle fibers, though the upstream cause differs considerably.
The Cinderella Hypothesis: Why Desk Work Causes Muscle Pain
One of the most clinically relevant findings from the trigger point literature is the role of sustained low-level contractions. According to Henneman's Size Principle, motor units are recruited in order from smallest to largest. During low-intensity tasks like typing, only the smallest motor units are activated. These "Cinderella" motor units (named because they are the first to start working and the last to rest) bear a disproportionate metabolic burden because they never rotate out, even though the task demands minimal overall force (Hagg, 1991).
Treaster and colleagues tested this concept directly in 16 female subjects performing computer work under varying postural and visual conditions. They found that high visual stress (small font, low contrast) was the primary factor associated with increased trigger point sensitivity in the upper trapezius, a finding that challenges the assumption that desk-related trigger points are mainly a postural problem (Treaster et al., 2006). Proper spinal alignment does not prevent trigger point development when the underlying mechanism is metabolic overload of specific motor units rather than structural misalignment.
Related What Causes Trigger Points? The Science of Muscle Overload and Six Competing Theories Related Trigger Point Dry Needling NYC: Conditions Treated and How It WorksDealing with Persistent Muscle Pain or Tightness?
Whether your pain stems from desk work, training, or an injury that has not resolved, our practitioners can identify the specific trigger points contributing to your symptoms and design a targeted treatment plan. We see patients with myofascial pain every day.
Schedule NowWhat Dry Needling May Do at the Biochemical Level
Given the biochemical complexity of the trigger point environment, one of the most significant findings from animal research is that dry needling may directly influence the chemical milieu at trigger point sites. In a rabbit model, Hsieh and colleagues found that a single dosage of dry needling at trigger spots increased beta-endorphin levels (an endogenous pain-relieving substance) in both the muscle and serum while reducing substance P (a pain-signaling neuropeptide) in the muscle and dorsal root ganglion. However, five dosages reversed these beneficial effects and instead increased concentrations of TNF-alpha, COX-2, HIF-1-alpha, iNOS, and VEGF in the muscle tissue, with these elevated levels persisting five days after treatment (Hsieh et al., 2012). This suggests that the biochemical response to dry needling is genuinely dosage-dependent, and that more needling does not necessarily produce more benefit.
These findings have practical implications for clinical dosing of dry needling. They support the idea that targeted, precise needling may produce a more favorable biochemical response than aggressive or excessive treatment. Clinical research also indicates that treating trigger points with dry needling is often accompanied by a local twitch response (LTR), which many practitioners consider a useful indicator that the needle has engaged the dysfunctional tissue, though the precise relationship between the LTR and clinical outcomes continues to be studied.
Beyond the Integrated Hypothesis: An Ongoing Scientific Debate
The integrated trigger point hypothesis is the most widely cited model, but the science is far from settled. At least six alternative hypotheses challenge different aspects of this framework. Quintner, Bove, and Cohen (2014) argue that the trigger point is not a primary muscle lesion at all, but rather a site of secondary allodynia driven by inflammation of peripheral nerves. Hocking (2010, 2013) proposes that the pathology is central, not peripheral: sustained plateau depolarizations in spinal motoneurons may maintain trigger points without any local endplate dysfunction. Gunn's radiculopathy model locates the primary problem at the nerve root. Srbely (2010) emphasizes segmental central sensitization. Jafri (2014) introduces a molecular pathway involving stretch-activated reactive oxygen species (X-ROS) that could amplify calcium dysregulation at the subcellular level.
What these competing models collectively suggest is that different patients may develop trigger points through different combinations of peripheral and central mechanisms. The practical implication, as Bialosky and colleagues have noted, is that manual therapy (including dry needling) likely works through combined biomechanical and neurophysiological pathways rather than any single mechanism in isolation (Bialosky et al., 2009).
Related What Causes Trigger Points? Six Competing Scientific Theories Explained in DepthWhat This Means for You
If you are living with chronic muscle pain, especially pain that seems to "travel," worsens with sustained postures, or does not respond well to anti-inflammatory medication alone, myofascial trigger points may be a contributing factor worth evaluating.
Key signs that your pain may have a myofascial component include: pain that is reproduced or worsened by pressing on a specific spot in a muscle; pain that radiates to a seemingly unrelated area when that spot is compressed; stiffness and restricted range of motion in the absence of joint pathology; and pain that developed after a period of overuse, sustained posture, or physical or emotional stress.
Because myofascial pain involves an interplay of local tissue biochemistry, motor endplate dysfunction, peripheral nociceptor sensitization, and in many cases central nervous system changes, effective treatment typically requires a targeted approach that addresses the trigger point directly. Dry needling, performed by a licensed acupuncturist or other qualified practitioner, is one of the most studied interventions for this purpose.
Related Myofascial Release NYC: Treatment for Pain, Stiffness, and Muscle Tightness Next in Series Part 2: What Causes Trigger Points? Muscle Overload and Competing Theories Continue Reading Part 3: Why Does Muscle Pain Spread? Peripheral Sensitization and Referred Pain Continue Reading Part 4: Why Chronic Pain Gets Worse Over TimeGet Expert Trigger Point Treatment at Morningside Acupuncture
At Morningside Acupuncture, we are the highest-rated acupuncture and dry needling clinic in New York City with over 500 five-star Google reviews. Our practitioners specialize in myofascial trigger point dry needling, sports acupuncture, and evidence-based pain management. If chronic muscle pain, referred pain, or unexplained tightness is affecting your daily life or performance, we can help.
Schedule NowReferences
- Bialosky, J.E., Bishop, M.D., Price, D.D., Robinson, M.E., & George, S.Z. (2009). The mechanisms of manual therapy in the treatment of musculoskeletal pain: A comprehensive model. Manual Therapy, 14(5), 531-538. https://doi.org/10.1016/j.math.2008.09.001
- Bron, C., & Dommerholt, J. (2012). Etiology of myofascial trigger points. Current Pain and Headache Reports, 16(5), 439-444. https://doi.org/10.1007/s11916-012-0289-4
- Chang, C.W., Chen, Y.R., & Chang, K.F. (2008). Evidence of neuroaxonal degeneration in myofascial pain syndrome: A study of neuromuscular jitter by axonal microstimulation. European Journal of Pain, 12(8), 1026-1030. https://doi.org/10.1016/j.ejpain.2008.01.012
- Fleckenstein, J., Zaps, D., Ruger, L.J., et al. (2010). Discrepancy between prevalence and perceived effectiveness of treatment methods in myofascial pain syndrome: Results of a cross-sectional, nationwide survey. BMC Musculoskeletal Disorders, 11(1), 32. https://doi.org/10.1186/1471-2474-11-32
- Gerwin, R.D., Dommerholt, J., & Shah, J.P. (2004). An expansion of Simons' integrated hypothesis of trigger point formation. Current Pain and Headache Reports, 8(6), 468-475. https://doi.org/10.1007/s11916-004-0069-x
- Hagberg, H. (1985). Intracellular pH during ischemia in skeletal muscle: Relationship to membrane potential, extracellular pH, tissue lactic acid and ATP. Pflugers Archiv: European Journal of Physiology, 404(4), 342-347. https://doi.org/10.1007/BF00585346
- Han, T.I., Hong, C.Z., Kuo, F.C., Hsieh, Y.L., Chou, L.W., & Kao, M.J. (2012). Mechanical pain sensitivity of deep tissues in children: Possible development of myofascial trigger points in children. BMC Musculoskeletal Disorders, 13, 13. https://doi.org/10.1186/1471-2474-13-13
- Harden, R.N., Bruehl, S.P., Gass, S., Niemiec, C., & Barbick, B. (2000). Signs and symptoms of the myofascial pain syndrome: A national survey of pain management providers. Clinical Journal of Pain, 16(1), 64-72. https://doi.org/10.1097/00002508-200003000-00010
- Hoeger Bement, M.K., & Sluka, K.A. (2014). The current state of physical therapy pain curriculum in the USA: A faculty survey. Journal of Pain, 16(2), 144-152. https://doi.org/10.1016/j.jpain.2014.11.001
- Hsieh, Y.L., Yang, S.A., Yang, C.C., & Chou, L.W. (2012). Dry needling at myofascial trigger spots of rabbit skeletal muscles modulates the biochemicals associated with pain, inflammation, and hypoxia. Evidence-Based Complementary and Alternative Medicine, 2012, 342165. https://doi.org/10.1155/2012/342165
- Jafri, M.S. (2014). Mechanisms of myofascial pain. International Scholarly Research Notices, 2014, 523924. https://doi.org/10.1155/2014/523924
- Kao, M.J., Han, T.I., Kuan, T.S., Hsieh, Y.L., Su, B.H., & Hong, C.Z. (2007). Myofascial trigger points in early life. Archives of Physical Medicine and Rehabilitation, 88(2), 251-254. https://doi.org/10.1016/j.apmr.2006.11.004
- Kuan, T.S., Hsieh, Y.L., Chen, S.M., Chen, J.T., Yen, W.C., & Hong, C.Z. (2007). The myofascial trigger point region: Correlation between the degree of irritability and the prevalence of endplate noise. American Journal of Physical Medicine & Rehabilitation, 86(3), 183-189. https://doi.org/10.1097/PHM.0b013e3180320ea7
- Shah, J.P., Phillips, T.M., Danoff, J.V., & Gerber, L.H. (2005). An in vivo microanalytical technique for measuring the local biochemical milieu of human skeletal muscle. Journal of Applied Physiology, 99(5), 1977-1984. https://doi.org/10.1152/japplphysiol.00419.2005
- Shah, J.P., Danoff, J.V., Desai, M.J., Parikh, S., Nakamura, L.Y., Phillips, T.M., & Gerber, L.H. (2008). Biochemicals associated with pain and inflammation are elevated in sites near to and remote from active myofascial trigger points. Archives of Physical Medicine and Rehabilitation, 89(1), 16-23. https://doi.org/10.1016/j.apmr.2007.10.018
- Simons, D.G. (2007). Orphan organ. Journal of Musculoskeletal Pain, 15(2), 7-9. https://doi.org/10.1300/J094v15n02_03
- Sluka, K.A., Radhakrishnan, R., Benson, C.J., et al. (2007). ASIC3 in muscle mediates mechanical, but not heat, hyperalgesia associated with muscle inflammation. Pain, 129(1-2), 102-112. https://doi.org/10.1016/j.pain.2006.09.038
Disclaimer: This web site is intended for educational and informational purposes only. Reading this website does not constitute providing medical advice or any professional services. This information should not be used for diagnosing or treating any health issue or disease. Those seeking medical advice should consult with a licensed physician. Seek the advice of a medical doctor or other qualified health professional for any medical condition. If you think you have a medical emergency, call 911 or go to the emergency room. No acupuncturist-patient relationship is created by reading this website or using the information. Morningside Acupuncture PLLC and its employees and contributors do not make any express or implied representations with respect to the information on this site or its use. For any legal interpretation of scope of practice in your state, consult a licensed attorney or regulatory authority.
Read more from our blog