How Does Dry Needling Work?
The science behind why inserting a thin acupuncture needle into a trigger point reduces pain and restores muscle function
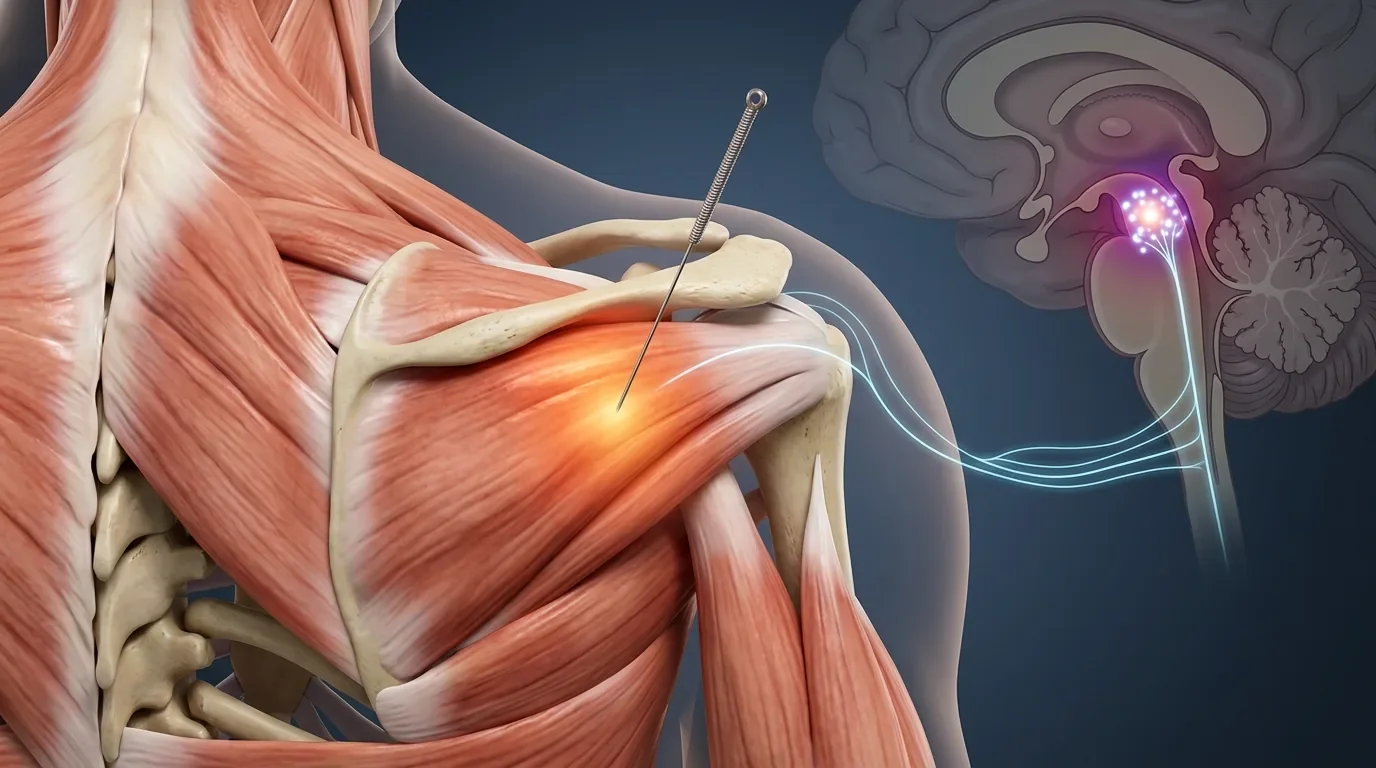
Dry needling works through several distinct mechanisms simultaneously: it mechanically disrupts the contracted muscle fibers at a trigger point, resets abnormal nerve signaling at the motor endplate, and reduces both the local chemical environment that drives pain and the broader central sensitization that amplifies it.
- The leading explanation for how trigger points form involves chronic dysfunction at the motor endplate, where excessive acetylcholine release causes sustained, involuntary muscle fiber contraction. Dry needling mechanically disrupts this process and restores normal electrical activity (Shah et al., 2015).
- Active trigger points create a local chemical environment elevated in inflammatory mediators including substance P, bradykinin, and TNF-alpha. These chemicals sensitize nearby nerve endings and can sustain pain even without ongoing tissue damage (Shah et al., 2015).
- Trigger points contribute to both peripheral sensitization, which lowers pain thresholds locally, and central sensitization, which causes pain signals to be amplified throughout the nervous system. Dry needling addresses both by removing a primary source of peripheral nociceptive input (Fernández-de-las-Peñas & Nijs, 2019).
- The local twitch response, a brief involuntary muscle contraction during needling, is associated with normalization of abnormal electrical activity at the trigger point and a rapid reduction in the concentration of pain-producing chemicals in the area (Fernández-de-las-Peñas & Dommerholt, 2018).
- Multiple systematic reviews confirm that dry needling is more effective than no treatment and, in many cases, more effective than sham needling for reducing pain and improving function across a range of musculoskeletal conditions (Gattie et al., 2017).
Want to understand if dry needling is appropriate for your pain?
Dry needling is most effective when the muscle is a significant driver of the pain, not when pain is primarily structural or neuropathic. At Morningside, we take the time to identify whether your pain is being driven by trigger points before recommending needling as part of your care.
Schedule NowStep One: The Target — What Dry Needling Is Actually Treating
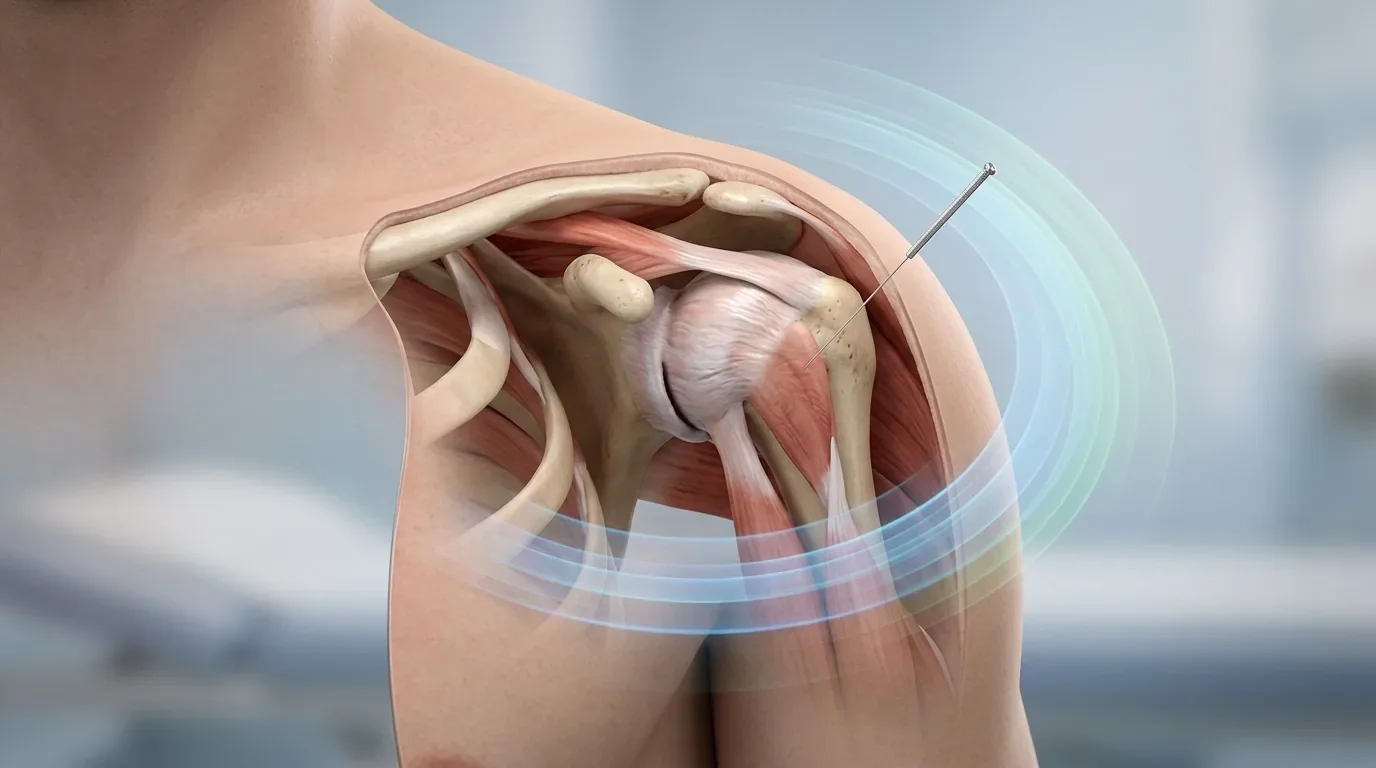
Before explaining how dry needling works, it helps to understand what it is working on. The primary target is the myofascial trigger point: a localized, hypersensitive nodule within a taut band of skeletal muscle. Trigger points are not simply tight muscles in a general sense. They represent a specific pathological state in a discrete cluster of muscle fibers, where the normal on-off signaling that controls contraction has become stuck in the "on" position.
An expert consensus definition from the international myofascial pain research community describes the trigger point by its hallmark features: a palpable taut band, a hypersensitive spot within that band, and a pattern of referred pain that travels predictably to sites away from the point itself (Fernández-de-las-Peñas & Dommerholt, 2018). Understanding that the pain a patient feels in their shoulder may originate from a trigger point in their neck muscle, or that leg pain may originate from a trigger point in the gluteus minimus, is fundamental to understanding why dry needling targets specific sites that may be remote from where the patient reports their pain.
Related What Is a Trigger Point? Understanding the Source of Referred PainThe Motor Endplate: Where the Problem Starts
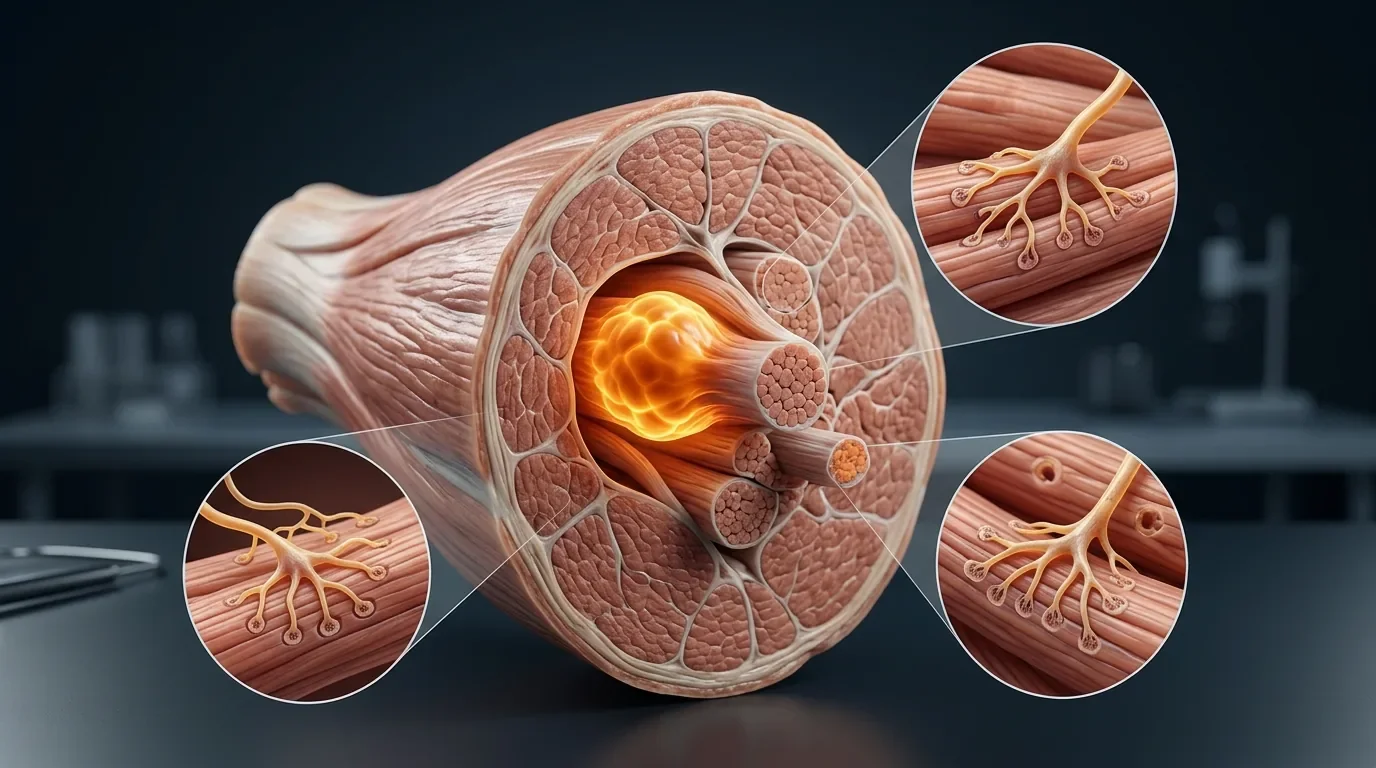
The most widely supported explanation for why trigger points form and persist is the integrated trigger point hypothesis. In a normally functioning muscle, each contraction is initiated by a nerve signal that causes the release of acetylcholine at the motor endplate, the junction between the motor nerve and the muscle fiber. When the signal ends, acetylcholine is quickly broken down by an enzyme called acetylcholinesterase, the muscle fiber relaxes, and the system resets.
In the trigger point model, this reset fails. Evidence from needle electromyography and microdialysis studies shows that trigger point locations exhibit abnormally high spontaneous electrical activity, indicating the motor endplate is releasing acetylcholine continuously rather than in controlled bursts (Shah et al., 2015). The result is a cluster of muscle fibers locked in continuous contraction. This ongoing metabolic demand, with inadequate blood flow to meet it, creates a hypoxic, acidic, inflammatory environment that sensitizes nearby nociceptors and generates both local tenderness and referred pain.
When an acupuncture needle penetrates the trigger point, it mechanically disrupts the contracted sarcomere structure at that site. The local twitch response, if it occurs, represents a brief spinal reflex that rapidly discharges the accumulated electrical activity at the endplate. Research confirms that after an LTR, the abnormal spontaneous electrical activity characteristic of the trigger point decreases markedly and the local concentrations of inflammatory chemicals fall (Fernández-de-las-Peñas & Dommerholt, 2018).
| Stage of the Cycle | What Goes Wrong | What Dry Needling Does |
|---|---|---|
| Motor endplate | Excess acetylcholine release; no reset | Mechanical disruption normalizes endplate activity |
| Sarcomere (muscle fiber) | Continuous involuntary contraction; taut band forms | LTR discharges accumulated tension; fiber releases |
| Local chemical environment | Elevated substance P, bradykinin, TNF-alpha, low pH | Post-LTR washout; inflammatory mediators reduce |
| Peripheral nociceptors | Sensitized by inflammatory milieu; pain threshold lowered | Reduced chemical sensitization; threshold normalizes |
| Spinal cord (dorsal horn) | Persistent nociceptive input drives central sensitization | Reduced peripheral input; dorsal horn excitability decreases |
| Brain (pain perception) | Amplified pain; hypersensitivity in referred zones | Less descending facilitation; referred pain and hyperalgesia reduce |
Peripheral and Central Sensitization: The Bigger Picture
Dry needling does not only affect the local muscle. Trigger points act as sustained sources of peripheral nociceptive input, and when that input is persistent enough, it alters how the spinal cord and brain process pain signals. This central sensitization is the state in which the nervous system becomes hyper-responsive: pain signals are amplified, areas of the body that are not injured begin to feel painful, and the normal mechanisms for dampening pain become less effective.
Research framing dry needling within a pain neuroscience framework has shown that needling reduces not only local muscle tenderness but also the broader pattern of altered pain processing that develops around a chronically active trigger point. By eliminating a primary driver of peripheral nociceptive signaling, dry needling helps the central nervous system gradually return to a less sensitized state (Fernández-de-las-Peñas & Nijs, 2019). This explains why patients with longstanding myofascial pain sometimes notice that distant areas of tenderness, not just the treated site, improve over a course of treatment.
Chronic muscle pain that keeps coming back?
Persistent pain that returns despite rest or massage is often maintained by centrally sensitized trigger points, not ongoing tissue damage. Understanding this distinction changes how treatment is approached. Morningside's practitioners are trained in pain neuroscience and will help you understand what is driving your specific pattern.
Schedule NowWhat the Evidence Shows About Clinical Effectiveness
The proposed mechanisms above are supported by biological research, but patients appropriately want to know whether these mechanisms translate into real-world outcomes. Systematic reviews and meta-analyses across multiple musculoskeletal conditions, including neck pain, shoulder pain, low back pain, and knee pain, consistently show that dry needling produces clinically meaningful reductions in pain and improvements in function (Gattie et al., 2017; Navarro-Santana et al., 2020).
Dry needling typically outperforms no treatment and sham (superficial, non-therapeutic) needling in the available trials. Whether it outperforms other active treatments depends heavily on the condition being treated. For myofascial-driven pain, particularly neck pain and shoulder girdle tension, it compares favorably to manual therapy, exercise, and corticosteroid injections in many studies. The advantage is most clear in conditions where the muscle itself is a primary pain driver rather than simply an affected secondary tissue.
Related Dry Needling Research — What the Clinical Evidence ShowsHow This Differs from Traditional Acupuncture
Dry needling and traditional acupuncture use the same sterile acupuncture needle, and the distinction between them is primarily one of diagnostic framework and anatomical target rather than the tool itself. Dry needling targets specific trigger points identified through palpation and a myofascial pain assessment. Traditional acupuncture styles select points based on a different diagnostic system, often involving patterns of pain, constitutional assessment, and classical point locations.
In practice, many of the effects described above, local mechanical disruption, neurophysiological modulation, and reduction of central sensitization, are also involved in traditional acupuncture analgesia. The mechanisms overlap considerably, which is why both approaches can produce meaningful clinical results. The choice of approach depends on the clinical presentation, the practitioner's training, and what the patient's pattern of pain suggests is driving the symptoms.
Related The Integrated Trigger Point Hypothesis — A Deeper Look at the ScienceSee how the science translates in practice
At Morningside Acupuncture, we are the highest-rated acupuncture and dry needling clinic in New York City with over 500 five-star Google reviews. We treat muscle-driven pain with a thorough understanding of the neuroscience behind trigger points and dry needling. If you have chronic pain that has not responded to other treatments, understanding the underlying mechanism may be the key to finding an approach that works.
Schedule NowFrequently Asked Questions
Does dry needling work the same way as injections?
No. Dry needling uses a solid acupuncture needle with no medication delivered. The effects are entirely mechanical and neurophysiological, not pharmacological. Trigger point injections use a hypodermic needle to deliver a substance (saline, local anesthetic, or corticosteroid) directly into the trigger point. Research comparing wet and dry needling has generally found comparable outcomes for trigger point pain, suggesting that the needle insertion itself, not the injectate, is the active component.
How quickly does dry needling start working?
Some patients notice immediate changes in muscle tension or pain distribution during or right after a session. Others notice improvement in the 24 to 72 hours following treatment as the inflammatory response resolves. For chronic conditions with central sensitization, meaningful change typically accumulates over several sessions rather than appearing dramatically after one. Progress should be noticeable by sessions 4 to 6.
Why does my pain come back between sessions at first?
In early treatment, the trigger point may partly reform between sessions, particularly if the conditions that generated it, postural loading, overuse, or stress, are still present. As treatment progresses and the underlying neuromuscular dysfunction is progressively resolved, recurrence between sessions typically diminishes. Complementary approaches that address the contributing factors, such as movement retraining or workstation modification, help extend the results of each session.
Is dry needling appropriate for all types of muscle pain?
Dry needling is most clearly indicated when myofascial trigger points are a primary driver of the pain. It is less relevant when pain is primarily structural (such as from a fractured bone), primarily neuropathic (from nerve root compression), or primarily inflammatory (such as active rheumatoid arthritis in the joint itself). A thorough assessment helps identify when trigger points are contributing substantially enough to make needling an appropriate part of the treatment plan.
References
- Shah, J. P., Thaker, N., Heimur, J., Aredo, J. V., Sikdar, S., & Gerber, L. H. (2015). Myofascial trigger points then and now: A historical and scientific perspective. PM&R, 7(7), 746–761. https://doi.org/10.1016/j.pmrj.2015.01.024
- Fernández-de-las-Peñas, C., & Dommerholt, J. (2018). International consensus on diagnostic criteria and clinical considerations of myofascial trigger points: A Delphi study. Pain Medicine, 19(1), 142–150. https://doi.org/10.1093/pm/pnx207
- Fernández-de-las-Peñas, C., & Nijs, J. (2019). Trigger point dry needling for the treatment of myofascial pain syndrome: Current perspectives within a pain neuroscience paradigm. Journal of Pain Research, 12, 1899–1911. https://doi.org/10.2147/JPR.S154728
- Gattie, E., Cleland, J. A., & Snodgrass, S. (2017). The effectiveness of trigger point dry needling for musculoskeletal conditions by physical therapists: A systematic review and meta-analysis. Journal of Orthopaedic & Sports Physical Therapy, 47(3), 133–149. https://doi.org/10.2519/jospt.2017.7096
- Navarro-Santana, M. J., Sanchez-Infante, J., Fernández-de-las-Peñas, C., Cleland, J. A., Martín-Casas, P., & Plaza-Manzano, G. (2020). Effectiveness of dry needling for myofascial trigger points associated with neck pain symptoms: An updated systematic review and meta-analysis. Journal of Clinical Medicine, 9(10), 3300. https://doi.org/10.3390/jcm9103300
Disclaimer: This web site is intended for educational and informational purposes only. Reading this website does not constitute providing medical advice or any professional services. This information should not be used for diagnosing or treating any health issue or disease. Those seeking medical advice should consult with a licensed physician. Seek the advice of a medical doctor or other qualified health professional for any medical condition. If you think you have a medical emergency, call 911 or go to the emergency room. No acupuncturist-patient relationship is created by reading this website or using the information. Morningside Acupuncture PLLC and its employees and contributors do not make any express or implied representations with respect to the information on this site or its use. For any legal interpretation of scope of practice in your state, consult a licensed attorney or regulatory authority.
Read more from our blog