What Is a Trigger Point?
A Plain-Language Guide to the Muscle Knots Behind Chronic Pain and Why They Refer Pain to Other Areas
Trigger points are hyperirritable spots within skeletal muscle that produce local pain, referred pain to distant areas, and measurable biochemical changes in the surrounding tissue. Understanding them is the foundation for understanding why dry needling and trigger point therapy work.
- A trigger point is a hyperirritable nodule within a taut band of skeletal muscle that, when compressed or stimulated, produces local tenderness and a predictable referred pain pattern to areas distant from the point itself (Fernández-de-Las-Peñas & Dommerholt, 2018).
- Active trigger points cause pain at rest and with movement; latent trigger points cause pain only when directly compressed but restrict movement and weaken the muscle even when not painful.
- The biochemical environment around an active trigger point contains significantly elevated concentrations of inflammatory mediators, neuropeptides, and catecholamines compared to normal muscle, confirming that trigger points are not merely tight spots but sites of genuine neurochemical disturbance (Shah et al., 2008).
- Trigger points form through a combination of acute overload, sustained low-level muscle contractions, posture-related compression, and neurological factors that sustain abnormal motor endplate activity (Bron & Dommerholt, 2012).
- Trigger points are extremely common. Systematic reviews have found active trigger points in the majority of patients presenting with spinal pain, neck pain, and shoulder pain, making them one of the most prevalent sources of musculoskeletal pain seen in clinical practice (Chiarotto et al., 2016).
- Dry needling and acupuncture directly target trigger points by provoking a local twitch response, releasing the taut band, and normalizing the local biochemical environment, producing both immediate and lasting pain reduction.
Do You Have Muscle Pain That Travels or Spreads?
Referred pain from trigger points is one of the most common sources of unexplained pain. Many patients are surprised to learn that their headaches originate in the neck and shoulders, or that their knee pain comes from the quadriceps. At Morningside Acupuncture, trigger point assessment and dry needling are at the center of how we approach musculoskeletal pain. We would be glad to help you identify what is actually driving your pain.
Schedule NowThe Simplest Definition
A trigger point is a localized, hyperirritable spot within a taut band of skeletal muscle. Press on it and you feel tenderness that is disproportionately sharp relative to the pressure applied. Sustain that pressure and you may feel pain radiating to a distant location, which is the referred pain phenomenon that makes trigger points so clinically interesting and so frequently missed.
The term and its systematic documentation come primarily from the work of Janet Travell and David Simons, whose two-volume Myofascial Pain and Dysfunction: The Trigger Point Manual, first published in 1983, catalogued the referred pain patterns of trigger points in virtually every skeletal muscle in the body. The patterns Travell and Simons described have been largely validated by subsequent research and remain the clinical roadmap used by practitioners today.
The formal definition that has emerged from international expert consensus identifies three diagnostic criteria as essential for a trigger point: a taut band within the muscle, a hypersensitive spot within that band, and referred pain elicited by compression of that spot (Fernández-de-Las-Peñas & Dommerholt, 2018). Some practitioners also use the local twitch response, a brief involuntary contraction of the taut band when needled or snapped with the fingers, as an additional confirmatory sign, though it is not required for diagnosis.
Related What Is Myofascial Pain Syndrome? Causes, Symptoms, and TreatmentActive and Latent: Two Varieties with Different Impacts
Not all trigger points behave the same way. The clinical distinction between active and latent trigger points is practically important because it shapes both the patient's experience and the treatment priority.
Active trigger points cause spontaneous pain, meaning pain that occurs without any pressure being applied to them. A person with an active trigger point in the upper trapezius may experience a constant ache at the base of the skull or behind the eye, even though the trapezius itself is nowhere near those locations. Active trigger points are tender to compression, but they are also symptomatic without it. They restrict the range of motion of the affected muscle, cause it to fatigue more quickly, and may inhibit surrounding muscles. Most patients who present with chronic musculoskeletal pain have at least some active trigger points contributing to their symptoms.
Latent trigger points, by contrast, do not produce spontaneous pain. A person who has latent trigger points in a muscle may not notice them until a practitioner presses on them, at which point the tenderness and referred sensation become apparent. Latent trigger points still restrict movement, cause weakness, and contribute to altered motor patterns, but they do so below the threshold of conscious pain in normal activity. Under conditions of stress, fatigue, illness, or sudden overload, latent trigger points can convert to active ones relatively quickly. This is why people who have been pain-free for months often report that a minor event, staying in an unusual position during a long flight, catching a cold, or a stressful week at work, "suddenly" triggered widespread pain. The trigger points were already there. The threshold shifted.
| Feature | Active Trigger Point | Latent Trigger Point | Plain English |
|---|---|---|---|
| Spontaneous pain | Present (without compression) | Absent (pain only on compression) | Active ones hurt on their own; latent ones only hurt when pressed |
| Referred pain | Reproduces patient's familiar pain pattern | May or may not produce referred sensation on pressure | Active TrPs are usually the ones behind your current symptoms |
| Effect on movement | Restricts range of motion; causes muscle weakness | Also restricts movement; contributes to altered motor patterns | Both types affect how the muscle moves, even when not painful |
| Conversion risk | May deactivate with treatment or rest | Can become active with overload, illness, or stress | Latent TrPs are primed to cause pain under the right circumstances |
| Treatment priority | Direct treatment needed to resolve symptoms | Worth treating to prevent flare-ups and improve function | Addressing latent TrPs reduces long-term recurrence |
What Is Actually Happening Inside a Trigger Point
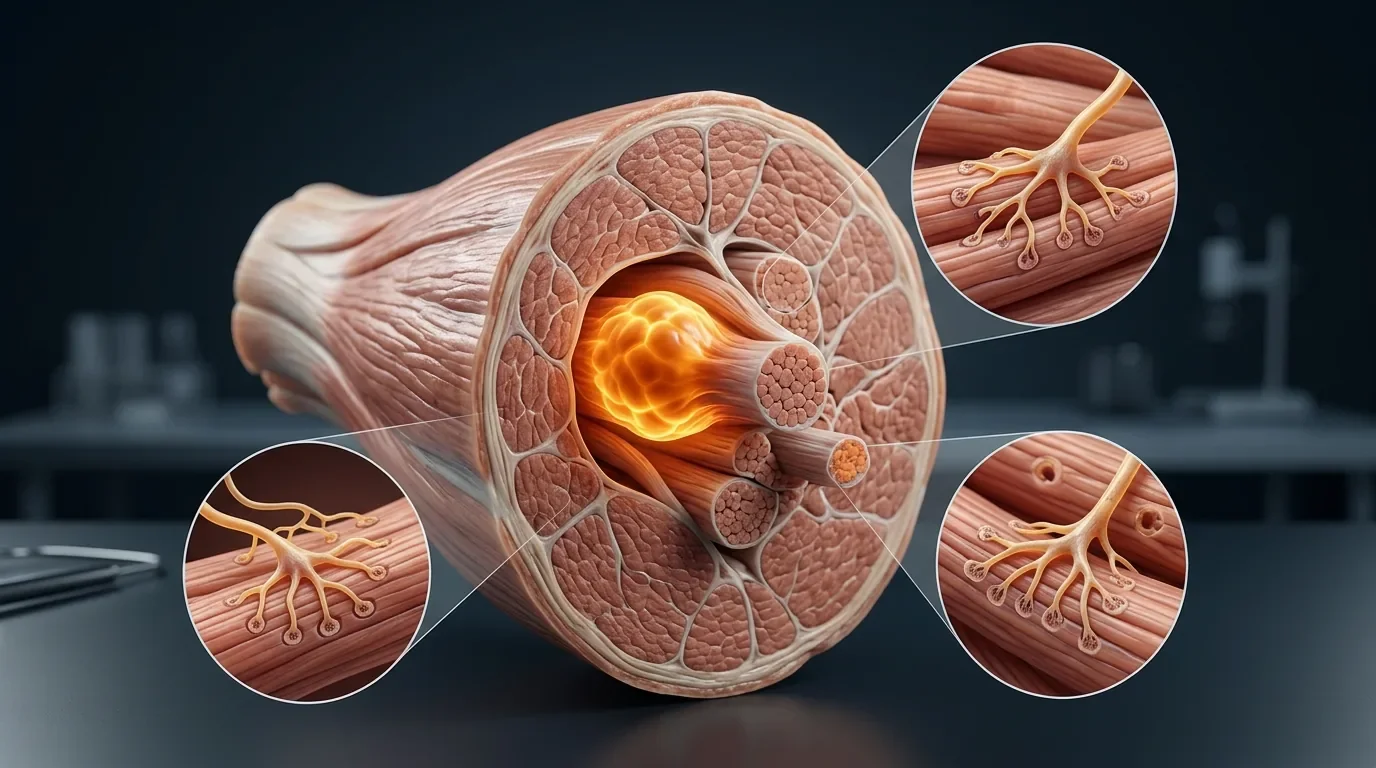
The traditional description of a trigger point as a "muscle knot" is a useful shorthand but understates the complexity of what is happening at a cellular and biochemical level. The most widely accepted explanation is the integrated trigger point hypothesis, which proposes that trigger points originate at dysfunctional motor endplates, the junctions where motor nerves meet muscle fibers.
At a normal motor endplate, nerve stimulation causes the release of acetylcholine, which crosses the junction and triggers muscle fiber contraction. After contraction, acetylcholine is broken down by the enzyme acetylcholinesterase, and the fiber relaxes. At a dysfunctional endplate, abnormal or excessive acetylcholine release causes sustained depolarization of the muscle fiber membrane, which generates persistent low-level contractile activity. This sustained contraction is not the same as a voluntary muscle contraction: it is a localized phenomenon occurring at the level of individual sarcomeres, the contractile units within muscle fibers, creating the characteristic taut band that can be palpated through the skin.
This sustained contraction has metabolic consequences. The contracted segment compresses local capillaries, restricting blood flow and oxygen delivery to the tissue. Without adequate oxygen, cellular metabolism shifts to anaerobic pathways, producing an accumulation of metabolic waste products and lowering local pH. The resulting acidic, poorly perfused environment activates nociceptors and promotes the release of inflammatory mediators, creating local tenderness and, through sensitization of adjacent sensory fibers, the referred pain patterns that are a hallmark of trigger point activity.
Shah and colleagues (2008) found that this biochemical milieu was not confined to the trigger point itself. Inflammatory mediators and neuropeptides were elevated at sites remote from the active trigger point as well, which may help explain why trigger points sensitize surrounding tissues, contribute to widespread pain, and can eventually promote central sensitization when they remain untreated over time.
Related Why Does Muscle Pain Spread? Referred Pain and Sensitization ExplainedChronic Muscle Pain That Hasn't Responded to Stretching or Rest?
Trigger points are persistent by nature, particularly when the conditions that created them, sustained posture, repetitive movement, or accumulated stress, continue unchanged. At Morningside Acupuncture, dry needling directly targets trigger points to produce the local twitch response that releases the taut band, normalizes the local biochemical environment, and interrupts the cycle that keeps trigger points active.
Schedule NowWhy Trigger Points Cause Pain Far from Where They Are
Referred pain is one of the most clinically important and counterintuitive aspects of trigger points. A trigger point in the infraspinatus muscle on the back of the shoulder refers pain to the front of the shoulder and down the inner aspect of the arm, a pattern that is often mistaken for rotator cuff pathology or cervical nerve root compression. A trigger point in the suboccipital muscles at the base of the skull refers pain across the top of the head and behind the eye, mimicking tension headache or migraine. A trigger point in the gluteus minimus refers pain down the outer leg in a pattern nearly indistinguishable from sciatica.
The mechanism of referred pain from trigger points involves the convergence of sensory input at the spinal cord. Nociceptive signals from the trigger point enter the spinal cord at a specific level, where they synapse with neurons that receive input from multiple body regions. When trigger point activity persistently sensitizes these spinal cord neurons, they begin interpreting input from all their convergent sources as painful. The brain, having no way to know the exact origin of the signal, attributes the pain to the region it learned is typically the source: the referred zone rather than the muscle where the trigger point actually lives.
This mechanism explains why treating pain at its reported location often fails when a trigger point is the actual driver. Injecting the shoulder or manipulating the cervical spine may provide temporary relief, but if a trigger point in the infraspinatus or scalenes is the generator, it will continue producing referred pain until addressed directly. Accurate trigger point assessment involves understanding these referral maps and working backward from the location of symptoms to the muscles most likely to contain the responsible trigger points (Gerwin, 2001).
What Causes Trigger Points to Form
Trigger points develop through a range of mechanisms, some obvious and some subtle. Direct acute trauma, such as a muscle strain or a sudden overload injury, is one common cause. The mechanical disruption of muscle fibers and motor endplates during acute injury sets up the conditions for dysfunctional endplate activity and the sustained contractile state that characterizes a trigger point.
Less obvious but extremely common is the development of trigger points through sustained low-level muscle activation, particularly in postural muscles that work continuously against gravity or against the positions imposed by desk work, screen use, and driving. Bron and Dommerholt (2012) reviewed the evidence for trigger point formation and identified sustained low-level contraction, rather than acute overload alone, as one of the most important contributing factors. Muscles asked to maintain continuous low-level activity never fully cycle through relaxation; their endplates remain chronically active, creating the conditions for trigger point development over time without a single identifiable injury.
Psychological stress is another established contributor. Stress activates the sympathetic nervous system, which increases muscle tone, reduces blood flow to musculature, and heightens nociceptor sensitivity. Prolonged stress does not injure muscles directly, but it creates a physiological environment in which muscles are more susceptible to trigger point formation and in which existing trigger points are maintained at a lower threshold for becoming symptomatic. This is why periods of high stress are often followed by flares of musculoskeletal pain, and why effective chronic pain management typically requires attention to stress alongside physical treatment.
| Cause | Mechanism | Common Examples | What This Means |
|---|---|---|---|
| Acute overload | Sudden mechanical disruption of muscle fibers and endplates | Muscle strain, sports injury, fall or impact | A single injury can initiate a trigger point that persists long after tissue heals |
| Sustained low-level contraction | Continuous endplate activity without full relaxation cycles | Desk work, keyboard/mouse use, driving, standing occupations | Even light work can create trigger points if maintained for hours without variation |
| Postural compression | Sustained pressure on muscles reducing local circulation | Leaning on armrests, prolonged sitting on wallet, tight straps | Compressive positions reduce oxygen delivery and promote trigger point conditions |
| Psychological stress | Sympathetic activation increasing muscle tone and reducing circulation | Work or life stress, anxiety, sleep deprivation | Stress amplifies trigger point sensitivity and can activate latent ones |
| Satellite and secondary trigger points | Referred pain or altered motor patterns from a primary trigger point creating new trigger points | Neck trigger points creating shoulder trigger points; shoulder trigger points creating arm trigger points | Untreated trigger points spread, making early treatment more efficient |
How Prevalent Are Trigger Points
Trigger points are remarkably common. A systematic review and meta-analysis by Chiarotto and colleagues (2016) examined the prevalence of trigger points across patients with spinal pain and found active trigger points in the large majority of individuals presenting with neck and low back pain. Studies in specific populations have found trigger points in a high proportion of patients with tension-type headache, shoulder pain, temporomandibular disorders, and chronic pelvic pain.
What makes this significant is how often these trigger points go unidentified as the primary pain generator. A patient presenting with chronic neck pain may receive imaging, which shows mild disc degeneration on MRI, and be told this is the cause of their pain. The disc finding may or may not be contributing. Active trigger points in the scalenes, sternocleidomastoid, and suboccipitals are almost certainly present, and they are generating or amplifying much of the symptom burden. When treatment focuses only on the structural imaging finding and ignores the trigger points, outcomes are often disappointing.
This is one of the reasons that trigger point assessment and dry needling have become central tools in evidence-informed musculoskeletal practice. The prevalence of trigger points in virtually every musculoskeletal pain population means that practitioners who are not looking for them are almost certainly missing a significant portion of the pain picture in most of the patients they treat.
Related Trigger Points Guide: Complete Reference for All Major MusclesTreatment: Why Trigger Points Need to Be Targeted Directly
Trigger points often do not resolve on their own, particularly when the mechanical, postural, or neurological conditions that generated them persist. Stretching the affected muscle can help temporarily by increasing blood flow and lengthening the taut band, but it does not address the dysfunctional motor endplate activity that maintains the trigger point. The same is true for heat, massage, and anti-inflammatory medication: each can reduce the symptomatic burden but typically does not deactivate the trigger point permanently.
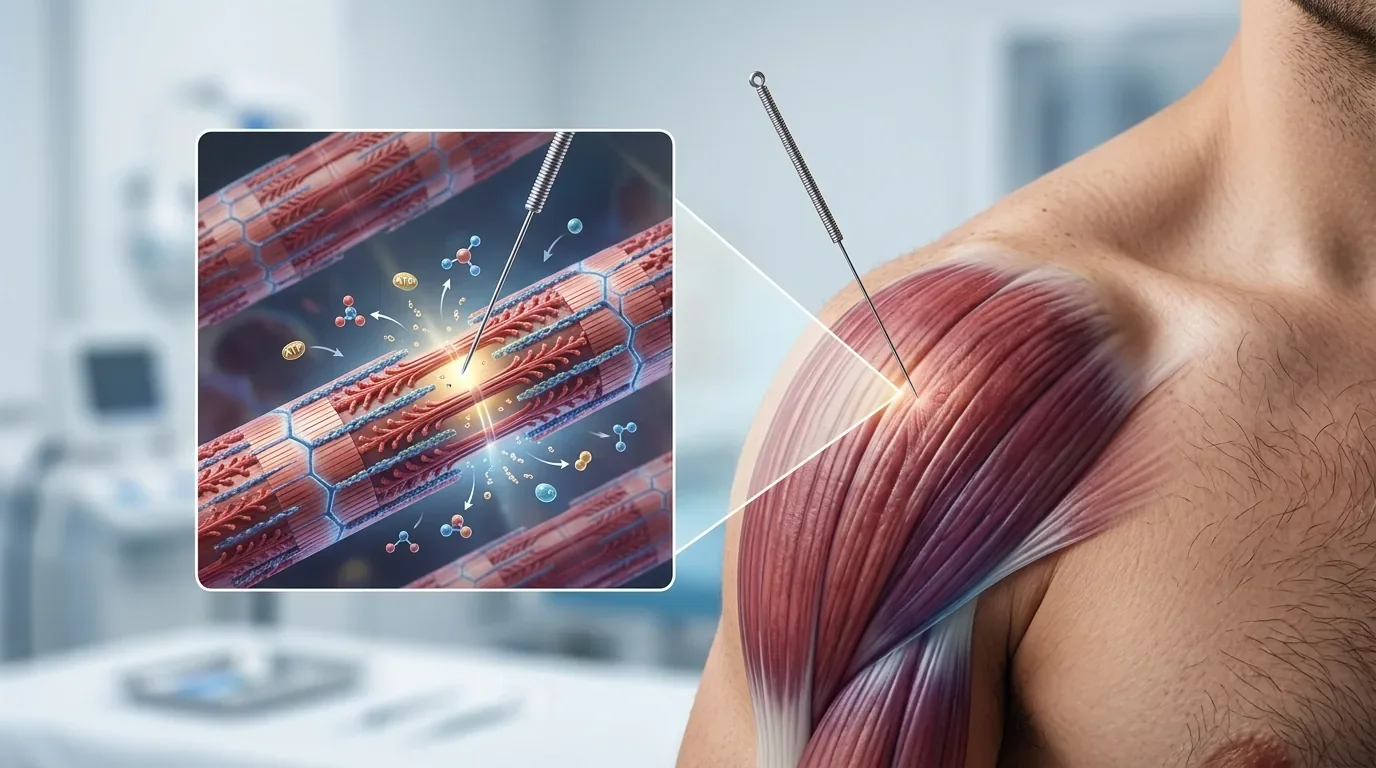
Dry needling, which involves inserting a thin acupuncture needle directly into the trigger point, is one of the most effective available treatments. The needle provokes a local twitch response, which is a brief, involuntary contraction of the taut band followed by relaxation. This twitch response appears to mechanically disrupt the dysfunctional endplate activity, rapidly reduces the concentration of inflammatory mediators in the local tissue, and is associated with immediate reduction in the local electrical activity that characterizes active trigger points. The post-needling soreness that some patients experience, typically lasting 24-48 hours, reflects the acute neurochemical response in the treated tissue and generally precedes lasting improvement in symptoms and function.
At Morningside Acupuncture, trigger point dry needling is integrated with broader assessment of the muscle chains and movement patterns that may be sustaining or re-creating trigger points over time. Needling a trigger point without addressing the underlying mechanical loading or postural factors tends to produce shorter-lived results. For lasting improvement, treatment needs to address both the trigger point itself and the conditions that generated it.
Ready to Identify and Treat the Trigger Points Behind Your Pain?
At Morningside Acupuncture, we are the highest-rated acupuncture and dry needling clinic in New York City with over 500 five-star Google reviews. Trigger point assessment and dry needling are central to our approach for chronic musculoskeletal pain, headaches, neck and shoulder pain, low back pain, and pain that has spread or refers to distant areas. Our practitioners are trained in the full range of trigger point patterns across the body, and we use this knowledge to work backward from your symptoms to the muscles most likely driving them. We would love to help you understand and resolve what is causing your pain.
Schedule NowFrequently Asked Questions
Are trigger points the same as muscle knots?
The term "muscle knot" is a common way patients describe what they feel, and it generally refers to the same phenomenon. Trigger points are the clinical term for hyperirritable spots within taut bands of muscle that cause tenderness and referred pain. The palpable firmness that patients and massage therapists describe as a "knot" corresponds to the taut band containing the trigger point. The underlying biology involves sustained contractile activity at individual muscle fiber contractile units, not an actual structural knot in the tissue.
Can trigger points heal on their own?
Latent trigger points may deactivate with adequate rest, stress reduction, and changes in the mechanical loading patterns that created them. Active trigger points, particularly those that have been present for months or years, are less likely to resolve without targeted treatment. The sustained endplate dysfunction that maintains them tends to be self-perpetuating, and the longer a trigger point is active, the more it sensitizes surrounding tissue and contributes to the central sensitization that can make pain chronic. Early treatment is generally more effective and requires fewer sessions than addressing long-established trigger points.
How does dry needling feel when you hit a trigger point?
When a needle contacts an active trigger point, most patients feel a distinctive deep ache or cramp in the muscle, sometimes accompanied by a twitching sensation in the muscle itself. This is the local twitch response and is considered a positive sign. The referred sensation, which may reproduce the patient's familiar pain pattern, often occurs simultaneously. The sensation during needling is brief, typically lasting seconds. The post-needling response, a dull muscular soreness similar to post-exercise soreness, may last 24-48 hours but is generally followed by meaningful improvement.
Are there trigger points in every muscle?
Any skeletal muscle is capable of developing trigger points, and trigger points have been documented in virtually every major skeletal muscle in the body. Some muscles, particularly postural muscles that work continuously against gravity and muscles involved in sustained occupational activities, develop trigger points more commonly. The upper trapezius, scalenes, levator scapulae, quadratus lumborum, piriformis, and suboccipitals are among the most frequently involved muscles in clinical practice. Our trigger points guide covers the referral patterns for all major muscles.
Does Morningside Acupuncture treat trigger points in all areas of the body?
Yes. We treat trigger points throughout the body, including the muscles of the neck, shoulders, back, hips, legs, and arms. Our practitioners are trained in the full library of trigger point referral patterns and assessment methods, allowing us to identify the muscles most likely responsible for your specific pain distribution. We use thin acupuncture needles and follow an evidence-based approach to dry needling that emphasizes both immediate trigger point release and strategies to prevent recurrence.
References
- Fernández-de-Las-Peñas, C., & Dommerholt, J. (2018). International consensus on diagnostic criteria and clinical considerations of myofascial trigger points: A Delphi study. Pain Medicine, 19(1), 142-150. https://doi.org/10.1093/pm/pnx207
- Shah, J. P., Danoff, J. V., Desai, M. J., Parikh, S., Nakamura, L. Y., Phillips, T. M., & Gerber, L. H. (2008). Biochemicals associated with pain and inflammation are elevated in sites near to and remote from active myofascial trigger points. Archives of Physical Medicine and Rehabilitation, 89(1), 16-23. https://doi.org/10.1016/j.apmr.2007.10.018
- Bron, C., & Dommerholt, J. D. (2012). Etiology of myofascial trigger points. Current Pain and Headache Reports, 16(5), 439-444. https://doi.org/10.1007/s11916-012-0289-4
- Gerwin, R. D. (2001). Classification, epidemiology, and natural history of myofascial pain syndrome. Current Pain and Headache Reports, 5(5), 412-420. https://doi.org/10.1007/s11916-001-0052-8
- Chiarotto, A., Clijsen, R., Fernandez-de-Las-Penas, C., & Barbero, M. (2016). Prevalence of myofascial trigger points in spinal disorders: A systematic review and meta-analysis. Archives of Physical Medicine and Rehabilitation, 97(2), 316-337. https://doi.org/10.1016/j.apmr.2015.09.021
Disclaimer: This web site is intended for educational and informational purposes only. Reading this website does not constitute providing medical advice or any professional services. This information should not be used for diagnosing or treating any health issue or disease. Those seeking medical advice should consult with a licensed physician. Seek the advice of a medical doctor or other qualified health professional for any medical condition. If you think you have a medical emergency, call 911 or go to the emergency room. No acupuncturist-patient relationship is created by reading this website or using the information. Morningside Acupuncture PLLC and its employees and contributors do not make any express or implied representations with respect to the information on this site or its use. For any legal interpretation of scope of practice in your state, consult a licensed attorney or regulatory authority.
Read more from our blog