Acupuncture for Postural Pain
Forward Head Posture, Upper Crossed Syndrome, Desk Worker Myofascial Patterns, and Why Needling the Cinderella Muscles Changes Everything
Postural pain from prolonged sitting, screen work, and sustained static loading is the most common musculoskeletal complaint in modern clinical practice. The muscles responsible are not simply "tight from bad posture"; they have developed myofascial trigger points through the Cinderella recruitment mechanism, making stretching and postural correction alone insufficient to resolve the symptom. Dry needling those trigger points directly changes the clinical picture.
- Postural pain from desk work and prolonged static postures develops through the Cinderella hypothesis: the low-threshold type I motor units in postural muscles are recruited first and derecruited last, so they remain continuously active during any sustained posture, eventually failing to maintain calcium homeostasis and developing myofascial trigger points (Simons et al., 1999).
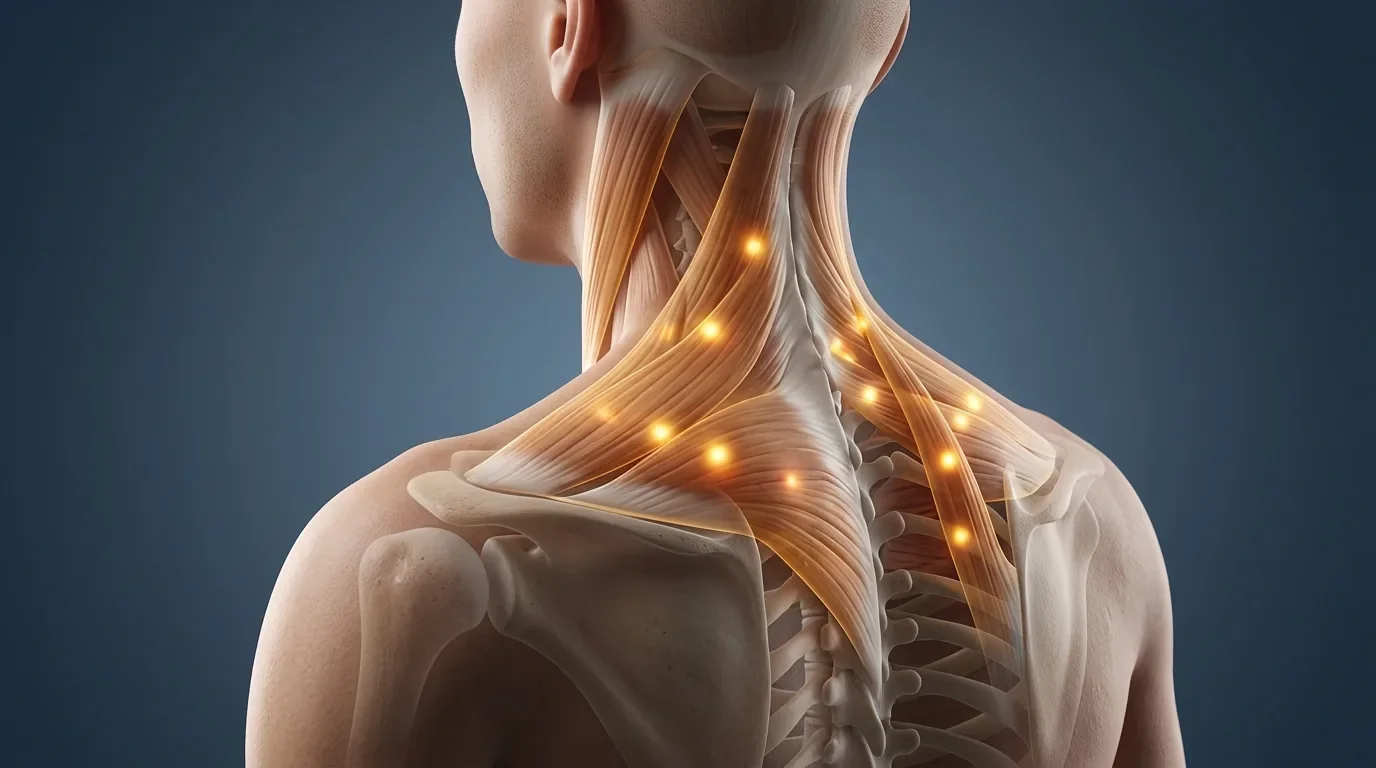
- Upper crossed syndrome (forward head, rounded shoulders, inhibited deep neck flexors and lower trapezius, overactive upper trapezius and pectoralis minor) is the most common postural pattern associated with neck, shoulder, and headache symptoms in desk workers.
- For every 2.5cm (approximately 1 inch) that the head translates forward of the center of gravity, the effective weight it places on the cervical spine increases by roughly 4.5kg; at a forward head of 7cm, the cervical spine may be managing the equivalent of a 27kg load instead of the 5kg it would manage in neutral alignment.
- Stretching and postural correction cannot eliminate established myofascial trigger points; the motor end plate dysfunction that maintains a trigger point requires a needle to resolve, and the taut band will not fully release with passive approaches alone (Kietrys et al., 2013).
- Acupuncture and dry needling of the specific trigger points maintaining postural pain (upper trapezius, levator scapulae, suboccipitals, rhomboids, pectoralis minor) produces immediate improvements in neck range of motion, shoulder mobility, and headache frequency that postural exercise alone cannot achieve rapidly.
- A large meta-analysis found acupuncture significantly superior to sham and no-treatment controls for chronic neck and upper back pain, with effect sizes that were maintained at 12-month follow-up (Vickers et al., 2018).
Neck, Shoulder, or Upper Back Pain from Desk Work That Won't Resolve?
Postural pain that persists despite stretching, ergonomic adjustments, and exercise usually has established trigger points in the postural muscles that require needling to resolve. At Morningside, dry needling of the upper trapezius, levator scapulae, suboccipitals, and pectoralis minor produces rapid improvements in the neck stiffness, shoulder tension, and headaches that characterize desk worker pain, typically within the first two to four sessions.
Schedule NowThe Cinderella Mechanism: Why Posture Causes Trigger Points
The Cinderella hypothesis (named for the last to leave the ball) explains why postural muscles develop trigger points more readily than phasic muscles under sustained loading. Motor unit recruitment follows the size principle: small, low-threshold type I (slow-twitch, oxidative) motor units are recruited first for low-force activities. In sustained postures, these same units remain continuously active because larger units are only recruited when force demands increase. The small type I units, designed for endurance, become trapped in prolonged activation without adequate recovery.
Under this sustained activation, the continuously firing motor end plates produce acetylcholine constantly, maintaining calcium release from the sarcoplasmic reticulum and sustaining sarcomere contraction beyond the point where ATP can maintain relaxation. The energetically depleted region develops into a trigger point: a hyperirritable nodule within a taut band, producing local and referred pain, reduced muscle extensibility, and impaired motor control.
This mechanism explains several clinical observations that puzzle patients. The pain is not simply proportional to the weight lifted; it correlates with the duration of sustained static postures. A two-hour meeting in a poor chair can produce more upper trapezius trigger point activity than a heavy weight-training session. The upper trapezius, levator scapulae, and rhomboids are essentially never "off" in desk workers who maintain sustained head and arm positions, and they develop trigger points despite performing no heavy work at all.
Related The Cinderella Hypothesis and Muscle PainUpper Crossed Syndrome: The Classic Postural Pain Pattern
Upper crossed syndrome (UCS), described by Vladimir Janda, identifies the characteristic muscle imbalance pattern of the head-forward, rounded-shoulder desk worker. The term reflects the X pattern of inhibited muscles (deep cervical flexors and lower trapezius) crossing with overactive muscles (upper trapezius/suboccipitals and pectoralis minor/major). Understanding this pattern guides treatment prioritization.
| Muscle | Status in UCS | Trigger Point Referral | Treatment Approach |
|---|---|---|---|
| Upper Trapezius | Overactive, shortened; dominant neck extensor; developing trigger points in classic "shoulder yoke" distribution | Lateral neck to temporal region; classic tension headache; ipsilateral ear and jaw | Primary dry needling target; most consistently responsible for tension headaches and neck pain in desk workers |
| Levator Scapulae | Overactive, shortened; elevates scapula and extends/rotates cervical spine; most commonly reported as "the kink in the neck" | Posterior lateral neck to the angle of the neck; restricted rotation ipsilaterally | Second most important dry needling target for desk worker neck pain; restriction of ipsilateral rotation is the characteristic finding |
| Suboccipitals | Chronically shortened by forward head; must continuously contract to maintain horizontal gaze when the head is forward; develop trigger points rapidly with screen work | Deep subcranial headache; pain behind the eye; band-like pressure around the head | Critical for resolving the deep subcranial headache component; dry needling at the base of the skull |
| Pectoralis Minor | Shortened by rounded shoulders; protracts and depresses the coracoid, contributing to thoracic outlet symptoms; trigger points refer to anterior chest and medial arm | Anterior chest pain; anterior shoulder; medial arm and ulnar hand (can mimic carpal tunnel) | Key anterior chain target; shortening drives the shoulder-rounding pattern; treating pectoralis minor improves scapular position and reduces anterior chain symptoms |
| Rhomboids | Inhibited and lengthened in rounded shoulders; may paradoxically develop trigger points from the sustained lengthened-position overload of maintaining scapular position against pectoralis minor tension | Medial border of the scapula; superficial diffuse mid-back aching between the shoulder blades | Important for the interscapular pain between the shoulder blades; often overlooked because the muscle feels sore rather than knotted |
| Scalenes | Overactive in forward head; compensate for deep cervical flexor inhibition; may compress brachial plexus between anterior and middle scalene (scalene triangle) producing upper extremity symptoms | Anterior chest; medial arm and forearm; may mimic carpal tunnel syndrome with hand numbness | Important when desk worker presents with arm or hand numbness; often the missing diagnosis in "carpal tunnel that hasn't responded to wrist treatment" |
Why Stretching Alone Doesn't Fix Postural Pain
The most consistent clinical observation in patients with established postural pain is that stretching provides temporary relief at best and fails to produce lasting change. Understanding why requires distinguishing between a muscle that is tight due to adaptive shortening (which stretching can address) and a muscle that has active trigger points (which stretching cannot resolve).
A trigger point involves a dysfunctional motor end plate maintaining sustained sarcomere contraction in a local region of the muscle. This is a neuromuscular phenomenon, not a structural one. Passive stretch lengthens the unaffected sarcomeres around the trigger point but cannot reset the dysfunctional end plate that maintains the contracted nodule. The taut band may soften momentarily under stretch, particularly after prolonged stretching, but the underlying motor end plate dysfunction persists and the trigger point returns to full activity within hours.
Dry needling directly disrupts the dysfunctional motor end plate by mechanically depolarizing the region through needle insertion, provoking a local twitch response that exhausts the accumulated acetylcholine and resets the end plate's resting firing behavior. The taut band resolves, the muscle returns to normal resting length, and the referred pain stops. Subsequent stretching and postural exercise then operate on muscle tissue that is genuinely extensible rather than on tissue whose extensibility is limited by motor end plate dysfunction.
Have You Been Stretching for Months Without Lasting Relief?
Established postural trigger points require needling to resolve, not stretching. At Morningside, we combine dry needling to eliminate the specific trigger points maintaining your postural pain with guidance on the exercises and ergonomic changes that will prevent them from recurring. The combination produces changes that neither approach achieves alone: rapid relief from needling, sustained improvement from the behavioral changes that follow.
Schedule NowLower Crossed Syndrome and Lumbar Postural Pain
The lower extremity equivalent of upper crossed syndrome is lower crossed syndrome: overactive hip flexors (iliopsoas and rectus femoris) and lumbar extensors crossing with inhibited gluteus maximus and abdominals. This pattern is driven by prolonged sitting, which holds the hip flexors in a shortened position and neurologically inhibits the gluteals through reciprocal inhibition.
The clinical consequence is that patients with sedentary occupations develop anterior pelvic tilt, increased lumbar lordosis, and chronic lower back pain from overloaded lumbar facets and paraspinal muscles. The psoas, quadratus lumborum, and piriformis develop trigger points from the sustained asymmetric loading that accompanies the altered pelvic position. Treating these trigger points, combined with hip extension strengthening to restore gluteal activation, addresses the lumbar component of desk worker postural pain.
Postural Pain from Desk Work in New York City
At Morningside Acupuncture, we are the highest-rated acupuncture and dry needling clinic in New York City with over 500 five-star Google reviews. We specialize in the specific myofascial patterns that develop from desk work, screen use, and sustained static postures, and we provide dry needling of the upper trapezius, levator scapulae, suboccipitals, pectoralis minor, and scalenes that are driving the neck pain, headaches, and shoulder tension you are living with. Schedule to finally address the muscles that your stretching routine has not been able to reach.
Schedule NowFrequently Asked Questions
Can bad posture cause chronic pain?
The relationship between posture and pain is more nuanced than the simple "bad posture causes pain" framing suggests. Static posture is a relatively poor predictor of pain when measured as a snapshot in time. What drives postural pain is the duration of sustained static loading in any position, which activates the Cinderella recruitment mechanism and leads to trigger point development in the postural muscles. The same neck position that is pain-free for 20 minutes may produce significant trigger point activity if maintained for 4 hours. It is the sustained static loading, more than any specific postural configuration, that generates the muscle pathology underlying postural pain.
How long does it take to relieve postural pain with dry needling?
Most patients with upper trapezius and levator scapulae trigger points notice meaningful improvements within two to four sessions. The first session typically produces immediate changes in neck range of motion and a reduction in the sense of tightness, followed by a variable period of soreness over 24-48 hours. Sessions two through four build on this, addressing deeper layers (suboccipitals, scalenes, pectoralis minor) and reducing the headache and arm symptom contributions. Lasting improvement requires concurrent changes in the sustained static loading patterns that are recreating the trigger points, particularly workstation ergonomics and movement frequency during desk work.
Why does my neck hurt more at the end of the workday?
The progressive worsening through the day reflects the Cinderella recruitment mechanism: the postural muscles (particularly upper trapezius and levator scapulae) begin the day with low trigger point activity, but after several hours of sustained desk posture they accumulate calcium dysregulation in the continuously recruited type I motor units, progressively developing more active trigger point activity. By the end of an 8-10 hour workday, these muscles are substantially more symptomatic than at the start. This is also why neck pain often improves over a long weekend or vacation and worsens rapidly upon returning to desk work.
Is a standing desk better for postural pain?
Standing desks reduce the hip flexor shortening of prolonged sitting and change the loading pattern on the lumbar spine, which may reduce lower back symptoms for some people. However, they do not eliminate the upper quarter postural pain of neck and shoulder muscles, because the arms-forward, head-forward position at a keyboard is nearly identical whether sitting or standing. Standing for prolonged periods also develops its own set of lower extremity and lower back postural trigger points. Alternating between sitting and standing (30-60 minute intervals), combined with movement breaks and dry needling of established trigger points, is more effective than either position exclusively.
What makes Morningside's approach to postural pain different?
Most postural pain treatment focuses on strengthening weak muscles and stretching tight ones, which addresses the muscle imbalance but does not eliminate the established trigger points that are producing the pain. At Morningside, we use dry needling to specifically target the motor end plate dysfunction in the trigger points that stretching cannot reach, producing immediate changes in pain and range of motion that exercise takes weeks or months to achieve. We then combine this with guidance on movement breaks, ergonomic positioning, and targeted exercises to prevent the trigger points from rapidly recurring. The combination is substantially more effective than either approach alone.
References
- Simons, D. G., Travell, J. G., & Simons, L. S. (1999). Travell & Simons' Myofascial Pain and Dysfunction: The Trigger Point Manual (2nd ed.). Williams & Wilkins.
- Vickers, A. J., Vertosick, E. A., Lewith, G., MacPherson, H., Foster, N. E., Sherman, K. J., Irnich, D., Witt, C. M., & Linde, K. (2018). Acupuncture for chronic pain: Update of an individual patient data meta-analysis. Journal of Pain, 19(5), 455-474. https://doi.org/10.1016/j.jpain.2017.11.005
- Kietrys, D. M., Palombaro, K. M., Azzaretto, E., Hubler, R., Schaller, B., Schlussel, J. M., & Tucker, M. (2013). Effectiveness of dry needling for upper-quarter myofascial pain: A systematic review and meta-analysis. Journal of Orthopaedic & Sports Physical Therapy, 43(9), 620-634. https://doi.org/10.2519/jospt.2013.4668
- Shah, J. P., Danoff, J. V., Desai, M. J., Parikh, S., Nakamura, L. Y., Phillips, T. M., & Gerber, L. H. (2008). Biochemicals associated with pain and inflammation are elevated in sites near to and remote from active myofascial trigger points. Archives of Physical Medicine and Rehabilitation, 89(1), 16-23. https://doi.org/10.1016/j.apmr.2007.10.018
- Zhao, Z. Q. (2008). Neural mechanism underlying acupuncture analgesia. Progress in Neurobiology, 85(4), 355-375. https://doi.org/10.1016/j.pneurobio.2008.05.004
- Qaseem, A., Wilt, T. J., McLean, R. M., & Forciea, M. A. (2017). Noninvasive treatments for acute, subacute, and chronic low back pain: A clinical practice guideline from the American College of Physicians. Annals of Internal Medicine, 166(7), 514-530. https://doi.org/10.7326/M16-2367
Disclaimer: This web site is intended for educational and informational purposes only. Reading this website does not constitute providing medical advice or any professional services. This information should not be used for diagnosing or treating any health issue or disease. Those seeking medical advice should consult with a licensed physician. Seek the advice of a medical doctor or other qualified health professional for any medical condition. If you think you have a medical emergency, call 911 or go to the emergency room. No acupuncturist-patient relationship is created by reading this website or using the information. Morningside Acupuncture PLLC and its employees and contributors do not make any express or implied representations with respect to the information on this site or its use. For any legal interpretation of scope of practice in your state, consult a licensed attorney or regulatory authority.
Read more from our blog