Reviewing the Pathophysiology of Chronic Pain
Chronic Pain Explained
A Systems-Level Mechanistic Framework to Explain Chronic Pain
Chronic pain is often discussed as if it were simply acute pain that never resolved. In reality, persistent pain represents a fundamental shift in how the nervous system processes sensory information. Once pain becomes chronic, it no longer functions as a warning signal of tissue damage. Instead, it reflects a maladaptive state involving altered neural excitability, impaired inhibitory control, immune activation, and long-term changes in brain organization.
A 2026 review published in the Clinical Journal of Pain synthesizes decades of research into a unified mechanistic model describing how pain transitions from an adaptive, protective response into a self-sustaining disorder. Rather than proposing a single cause, the authors describe chronic pain as a dynamic cascade that unfolds across peripheral tissues, the spinal cord, the brain, the immune system, and psychosocial context.
Understanding this cascade helps explain why pain often persists despite “normal” imaging, why symptoms spread or change over time, and why effective treatment frequently requires addressing more than one level of the system.
Key Points
Chronic pain is not prolonged acute pain; it represents a qualitatively different neurophysiological state
Pain chronification develops through interacting and reinforcing mechanisms, not a linear sequence
Peripheral input, central amplification, immune signaling, and psychosocial stressors shape pain together
Nervous system plasticity allows pain to become embedded in sensory, emotional, and cognitive networks
Treatment effectiveness depends on matching interventions to the dominant mechanisms present
Chronic Pain Explained in Plain English
| Concept | Plain-English Meaning | What You Might Notice | Why It Matters |
|---|---|---|---|
| Acute pain vs. chronic pain | Acute pain is an alarm that helps protect you while tissues heal. Chronic pain is when the alarm system stays on too long and becomes overprotective. | Pain lasts longer than expected, even when the original injury seems “healed.” | Chronic pain often needs nervous-system-focused care, not just tissue-focused care. |
| Peripheral sensitization | The nerves in the painful area become extra reactive, like a smoke detector that goes off too easily. | Tenderness, sharper pain with pressure, pain that flares with activity or after stress. | Ongoing “extra loud” signals from the area can keep the pain system turned up. |
| Central sensitization | The spinal cord and brain start amplifying pain signals, so the volume knob is turned up. | Pain spreads, feels disproportionate, or is triggered by light touch or normal movement. | Pain may continue even when tissue damage is minimal or no longer present. |
| Reduced inhibition | The body’s “brakes” on pain don’t work as well, so pain signals get through more easily. | Pain is harder to calm down once it starts; more frequent flare-ups. | Improving inhibitory control is often a key goal in treatment. |
| Descending modulation | Your brain normally turns pain signals up or down depending on context. In chronic pain, this control system can become less effective. | Stress, poor sleep, and mood changes strongly affect pain levels. | This explains why treating sleep, stress, and regulation can improve pain. |
| Maladaptive neuroplasticity | The nervous system “learns” pain patterns over time, and pain becomes linked to emotions, attention, and threat detection. | Fear of movement, feeling “stuck,” increased body tension, persistent sensitivity. | These patterns can change, but they often need consistent, multi-layered treatment. |
| Neuro-immune signaling | The immune system and nervous system talk to each other. In chronic pain, that conversation can keep nerves irritated. | Inflammatory flare-ups, widespread aches, fatigue, or symptoms that don’t match imaging. | Reducing inflammatory load and improving recovery inputs may help calm pain sensitivity. |
| Psychosocial factors (biological effects) | Stress, trauma, low sleep, and adversity can change your biology (hormones, neurotransmitters, immune signals), not just your mindset. | Pain worsens during high-stress periods; mood and pain feel tightly linked. | Addressing these factors is not “in your head,” it’s part of nervous system care. |
| Why imaging can be “normal” | Pain can be driven by sensitized nerves and amplified processing, even without a major structural finding. | “MRI looks fine” but pain persists; symptoms vary day to day. | It helps explain why pain can be real and severe even when imaging is not dramatic. |
How Pain Normally Resolves
Under healthy conditions, nociception is time-limited. Tissue injury activates peripheral nociceptors, signals travel through the spinal cord to the brain, and protective behaviors follow. As healing occurs, inflammatory mediators decrease, nociceptor thresholds normalize, and descending inhibitory pathways help quiet residual signaling.
This resolution depends on two key processes:
Reduction of peripheral nociceptive drive
Intact central inhibition and adaptive plasticity
Chronic pain emerges when these processes fail.
Plain-English summary:
Normally, pain turns on to protect you and then turns off once healing occurs. Chronic pain begins when the body’s “alarm system” doesn’t fully shut down and the nervous system stays stuck in a heightened state.
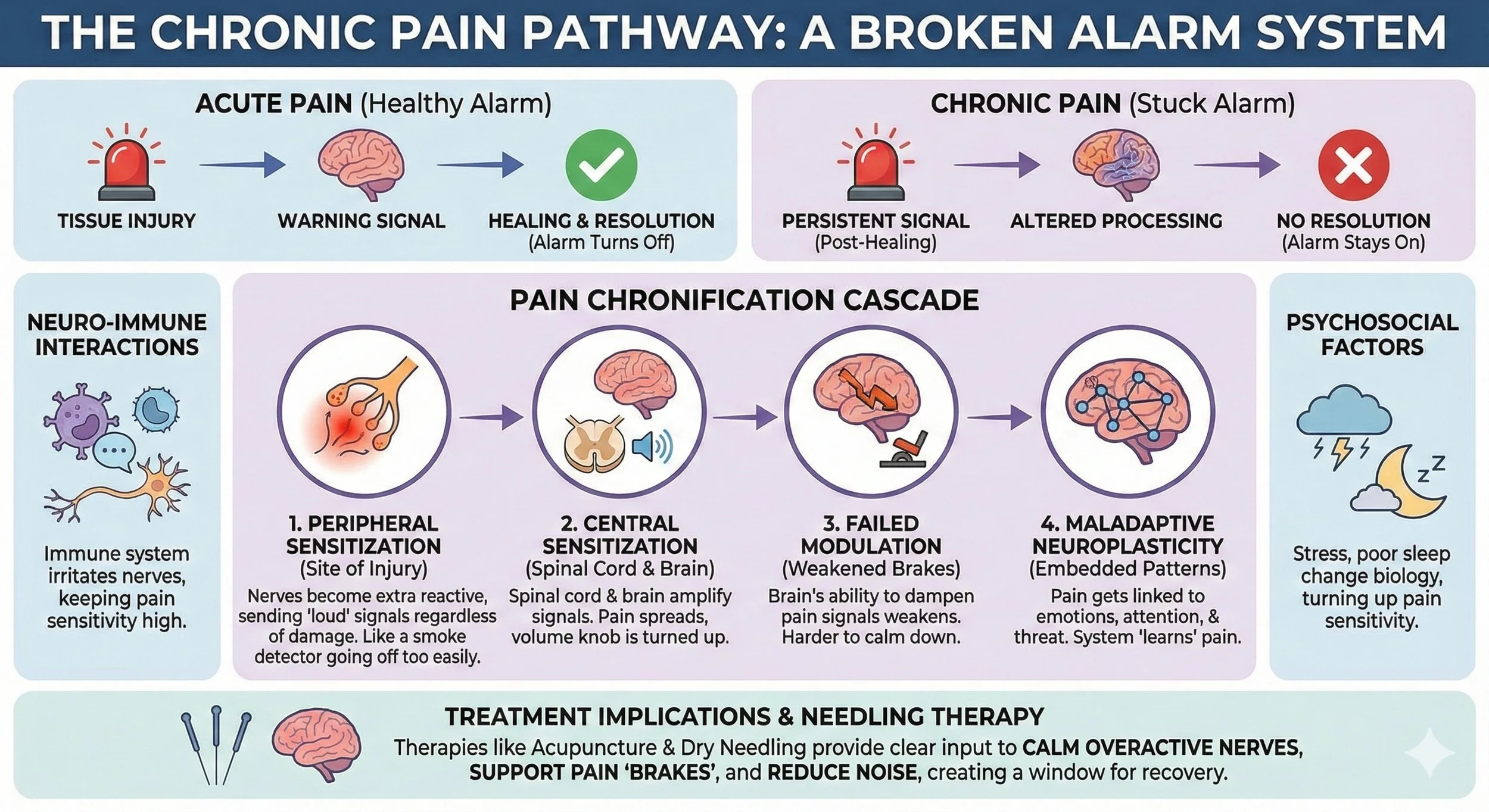
Stage 1: Peripheral Sensitization – When the Alarm Becomes Overreactive
The chronification process often begins at the site of injury or inflammation. Following tissue stress, inflammatory mediators, growth factors, and ion-channel changes alter the excitability of nociceptors. These sensory neurons begin responding more strongly to mechanical or chemical input and may fire in response to stimuli that were previously non-painful.
Crucially, this is not just increased signaling; it is altered signal encoding. Sensitized nociceptors provide stronger, more frequent input to the spinal cord, increasing the likelihood that central circuits adapt in response.
Clinically, this stage may present as localized tenderness, movement-related pain, or sensitivity that feels disproportionate to tissue findings. If peripheral sensitization persists, it can act as a continuous driver for deeper neural changes.
Plain-English summary:
The nerves in the painful area become overly sensitive, like a car alarm that goes off too easily. Even normal movement or pressure can feel threatening, and these “extra loud” signals keep feeding the nervous system.
Stage 2: Central Sensitization – Amplification Within the Spinal Cord and Brain
Sustained nociceptive input can induce plastic changes within the central nervous system. Neurons in the dorsal horn of the spinal cord become more excitable, synaptic transmission is strengthened, and inhibitory neurotransmission becomes less effective. Glial cells, once thought to be passive support cells, actively contribute by releasing substances that further enhance neuronal firing.
This stage is marked by gain amplification. Pain signals are no longer transmitted proportionally to input; instead, the system becomes biased toward excitation. Importantly, pain may now persist even if peripheral input decreases.
From a clinical standpoint, central sensitization helps explain:
Pain spread beyond the original injury
Heightened responses to touch or movement
Symptoms that fluctuate independently of tissue status
At this point, pain has become less about damage and more about processing.
Plain-English summary:
The spinal cord and brain turn the volume knob up on pain. Pain can spread, feel excessive, or stick around even when the original injury has improved.
Stage 3: Failure of Descending Pain Modulation
In a healthy nervous system, the brain continuously modulates incoming sensory signals. Descending pathways can dampen nociceptive input based on context, expectation, and perceived threat. In chronic pain, this balance is disrupted.
Inhibitory systems may become less effective, while facilitatory pathways remain active or dominant. Neurochemical changes reduce the brain’s ability to suppress nociceptive transmission, allowing amplified signals to reach conscious perception more easily.
This loss of modulation does not simply increase pain intensity; it removes flexibility. The system becomes less capable of adapting to changing sensory demands, stressors, or movement.
Plain-English summary:
The brain’s pain “brakes” stop working as well. Stress, poor sleep, or movement can trigger pain more easily because the system has lost its ability to calm itself down.
Stage 4: Maladaptive Neuroplasticity and Pain Embedding
Over time, chronic pain becomes embedded within broader brain networks. Neuroimaging studies show altered connectivity and structural changes in regions involved in sensory processing, emotion, attention, and memory. Pain is no longer processed in isolation but becomes linked to threat detection, mood regulation, and cognitive appraisal.
This stage helps explain why pain is often accompanied by:
Emotional distress
Cognitive fatigue
Heightened vigilance or fear of movement
Importantly, these changes are plastic, not fixed, but they are reinforced through repeated experience.
Plain-English summary:
Pain becomes learned by the nervous system and intertwined with emotions, attention, and fear. The pain feels more persistent and exhausting, but the system is still capable of change with the right inputs.
Putting It All Together
Chronic pain develops when the body’s normal pain alarm system fails to fully shut off after an injury. Over time, local nerves become overly sensitive, the spinal cord and brain amplify incoming signals, and the brain’s ability to calm pain down becomes less effective. As pain persists, it becomes embedded in wider brain networks involved in stress, emotion, and threat detection, making symptoms feel more widespread and unpredictable. Immune signaling, poor sleep, stress, and repeated flare-ups reinforce this cycle, even when tissue healing has occurred. The good news is that these changes are learned and adaptable, which means the nervous system can improve when treatment addresses the right mechanisms in the right way.
Neuro-Immune Interactions: Sustaining the Pain State
Immune signaling plays a critical role throughout the cascade. Peripheral immune cells, spinal glia, and central inflammatory mediators influence neuronal excitability and synaptic function. These interactions blur the traditional boundary between immune and nervous systems.
Emerging research suggests that systemic immune factors, including those influenced by the gut microbiome, may further shape pain vulnerability by altering inflammatory tone and metabolic signaling.
This immune involvement helps explain why chronic pain often overlaps with fatigue, mood disorders, and other systemic symptoms.
Plain-English summary:
The immune system and nervous system constantly talk to each other, and in chronic pain that conversation can keep nerves irritated and reactive. This helps explain why people with chronic pain often feel worn down, inflamed, or “off” in ways that go beyond just pain.
Psychosocial Factors as Biological Modulators
Psychological stress, trauma exposure, sleep disruption, and social adversity are not merely “contributors” to chronic pain. They actively modify neuroendocrine and neurotransmitter systems involved in pain regulation. Stress hormones influence immune activity, synaptic plasticity, and descending inhibition.
Over time, these influences may become biologically embedded through epigenetic mechanisms, altering gene expression and nervous system responsiveness. This integration of experience and biology explains why pain trajectories vary so widely between individuals with similar injuries.
Plain-English summary:
Stress, poor sleep, and past experiences don’t just affect how pain feels mentally, they change how the body and nervous system work. These factors can “turn up” pain sensitivity at a biological level, which is why two people with the same injury can have very different outcomes.
Integrating the Cascade: A Nonlinear, Self-Reinforcing System
The key insight of this framework is that chronic pain does not progress in a straight line. Peripheral sensitization can maintain central changes. Central amplification can heighten peripheral sensitivity. Stress can worsen immune activation, which further alters neural signaling.
Once established, the system sustains itself unless multiple reinforcing loops are addressed.
Plain-English summary:
Chronic pain feeds on itself through multiple feedback loops. Pain makes the nervous system more sensitive, which leads to more pain, unless treatment interrupts several parts of the cycle at once.
Plain-English Summaries: Chronic Pain Mechanisms (Quick Reference)
| Section | Plain-English Summary | What It Can Feel Like | Key Takeaway |
|---|---|---|---|
| How Pain Normally Resolves | Pain is meant to turn on to protect you, then turn off as healing finishes. Chronic pain starts when the alarm system doesn’t fully shut down. | Pain lingers longer than expected, even after the original injury seems better. | Chronic pain often reflects a “stuck” alarm system, not just ongoing tissue damage. |
| Stage 1: Peripheral Sensitization | Nerves in the painful area become overly reactive, sending louder signals to the nervous system. | Local tenderness, sharp pain with pressure, flares after activity. | Overreactive local nerves can keep feeding the pain cycle. |
| Stage 2: Central Sensitization | The spinal cord and brain amplify pain signals, like the volume knob is turned up. | Pain spreads, feels disproportionate, sensitivity to touch or movement. | Pain can persist even when the original tissue problem improves. |
| Stage 3: Descending Modulation Failure | The brain’s pain “brakes” don’t work as well, so it’s harder to calm pain once it starts. | Stress and poor sleep trigger flares; pain is harder to settle down. | Improving regulation and inhibitory control becomes a key treatment target. |
| Stage 4: Maladaptive Neuroplasticity | Pain becomes learned and linked with attention, emotion, and threat detection networks. | Fear of movement, persistent sensitivity, mental fatigue. | These patterns can improve, but usually need consistent retraining inputs. |
| Putting It All Together | Chronic pain is a chain reaction: local sensitivity builds, the nervous system amplifies signals, brakes weaken, and pain becomes embedded. Immune and stress systems can reinforce the loop, but the nervous system can adapt in a healthier direction. | Ups-and-downs, flare cycles, symptoms that don’t match imaging. | The goal is to interrupt multiple parts of the cycle, not chase one “source.” |
| Neuro-Immune Interactions | The immune and nervous systems can keep each other activated, sustaining sensitivity. | Fatigue, systemic flares, pain that feels inflammatory or widespread. | Immune signaling can maintain pain sensitivity even after tissues heal. |
| Psychosocial Factors as Biological Modulators | Stress, trauma, and poor sleep change biology (hormones, neurotransmitters, immune signals), not just mindset. | Pain worsens during stressful periods; sleep and mood strongly affect symptoms. | Addressing stress and sleep is part of nervous system care, not “in your head.” |
| Integrating the Cascade | Chronic pain is a self-reinforcing loop: sensitivity increases pain, and pain increases sensitivity, unless multiple loops are interrupted. | Recurring flare-ups; progress stalls if only one factor is treated. | Multi-layered treatment works best because the system reinforces itself. |
Where Acupuncture and Dry Needling May Help with Chronic Pain
Acupuncture and dry needling involve the use of a solid filiform acupuncture needle to mechanically and neurophysiologically interact with tissue and nervous system function. From a mechanistic perspective, needling-based interventions may influence several points within the chronification cascade.
At the peripheral level, needling may alter local nociceptor sensitivity, tissue stiffness, and inflammatory signaling. Reducing ongoing peripheral input can be particularly relevant when peripheral sensitization continues to drive central changes.
At the spinal and supraspinal levels, sensory input generated by needling may engage segmental reflexes and descending modulatory systems, potentially supporting inhibitory control. These effects are not isolated to pain intensity but may also influence motor output, muscle activation patterns, and sensory-motor integration.
Within a broader treatment plan, acupuncture and dry needling may help reduce nociceptive load, normalize altered neural signaling, and create conditions that support adaptive neuroplasticity.
Plain-English summary:
Acupuncture and dry needling use very thin needles to give the nervous system clear, targeted input. This input can help calm overly sensitive local nerves, reduce ongoing “noise” coming from irritated tissues, and support the brain’s ability to turn pain signals down. When used as part of a larger treatment plan, needling can make the nervous system less reactive and create a window where movement, strength work, and recovery strategies work better and last longer.
How Acupuncture and Dry Needling May Help in Chronic Pain
| Part of the Chronic Pain Cascade | What’s Happening | How Needling-Based Therapy May Relate | What This Can Look Like Clinically |
|---|---|---|---|
| Peripheral sensitization | Local nerves become overly reactive and tissues can feel tender, guarded, and stiff. | Acupuncture and dry needling use a solid filiform acupuncture needle to create controlled sensory input and local mechanical stimulation, which may help reduce sensitivity and normalize local signaling. | Reduced tenderness, improved ease of movement, less “protective tightness,” faster calm-down after activity. |
| Persistent nociceptive drive | Ongoing input from irritated tissues keeps feeding the spinal cord and brain. | By decreasing local irritability and improving tissue tolerance, needling may help reduce the volume of incoming signals that maintain the cycle. | Fewer flare-ups, less constant background ache, better tolerance to rehab and strength work. |
| Central sensitization | The nervous system amplifies pain and spreads sensitivity beyond the original area. | Needling may influence spinal segmental processing and engage descending inhibitory pathways, potentially shifting the system away from constant amplification. | Less pain spread, less sensitivity to touch, improved ability to tolerate normal movement. |
| Reduced inhibition (“brakes” are weaker) | Pain-calming circuits are less effective; the system is biased toward excitation. | Acupuncture-style dosing and electroacupuncture may support inhibitory modulation and autonomic regulation, which can be relevant when pain is stuck in a high-alert state. | Improved recovery between workouts, fewer “wired but tired” patterns, better sleep-related improvements. |
| Motor control changes + guarding | Muscles may stay guarded, inhibited, or overactive as part of protection. | Dry needling is an acupuncture style that often targets myofascial trigger points and sensitized muscle regions, which may help reduce guarding and improve recruitment when combined with exercise. | Better muscle activation, less cramping/tightness, improved movement quality during rehab drills. |
| Stress physiology and pain modulation | Stress, sleep disruption, and mood changes can amplify pain through neuroendocrine and immune pathways. | Acupuncture may support autonomic balance and downshift hyperarousal, which can indirectly improve pain sensitivity and recovery capacity. | Less stress-linked pain spikes, better sleep, improved resilience during busy periods. |
| Long-term neuroplasticity | Pain becomes learned and reinforced across networks involving attention, threat, and memory. | Needling alone is rarely the whole answer, but it can create a window of reduced sensitivity that makes graded exposure, strength training, and nervous system retraining easier and more tolerable. | More progress with rehab, fewer setbacks, improved confidence with movement. |
Clinical Implications
This framework reinforces the idea that chronic pain requires mechanism-informed care. Treatments that address only tissue structure may fall short when pain is driven by altered neural processing. Conversely, interventions that reduce peripheral drive or improve modulation may have downstream effects on central sensitization.
Understanding where a patient sits within the cascade can help guide treatment selection, expectations, and pacing.
Conclusion
Chronic pain is best understood as an emergent property of interacting biological, neural, immune, and psychosocial systems. The framework presented in this review provides a cohesive explanation for why pain persists beyond healing, why symptoms vary between individuals, and why effective care often requires addressing more than one layer of the system.
By shifting the focus from isolated tissues to dynamic systems, this model offers a clearer path toward individualized, evidence-informed pain management.
Frequently Asked Questions (FAQ)
What is chronic pain, and how is it different from acute pain?
Chronic pain is pain that persists beyond expected tissue healing time and often reflects changes in how the nervous system processes pain signals. Acute pain is protective and typically improves as tissues heal, while chronic pain can persist due to sensitization, reduced inhibition, and altered pain modulation.
Can chronic pain happen even if imaging is normal?
Yes. Chronic pain can be driven by sensitized nerves and amplified processing in the spinal cord and brain, which may not show up on MRI or X-ray. Imaging can be useful, but it doesn’t always explain pain intensity or persistence.
What is peripheral sensitization in chronic pain?
Peripheral sensitization means that pain-sensing nerves in the affected area become more reactive due to inflammatory mediators and ion-channel changes. This can make tissues feel tender and can increase pain responses to pressure or movement.
What is central sensitization, and how do you know if you have it?
Central sensitization occurs when the spinal cord and brain amplify pain signals. Signs may include widespread pain, pain that feels disproportionate, sensitivity to light touch, pain that lingers after activity, and symptoms that fluctuate with stress or sleep.
Why does stress make chronic pain worse?
Stress can shift the nervous system into a high-alert state, affecting neurotransmitters, hormones, and immune signaling that modulate pain sensitivity. This can reduce your ability to “turn down” pain signals and increase vulnerability to flare-ups.
Can acupuncture help chronic pain?
Acupuncture uses a solid filiform acupuncture needle and may help regulate pain processing by influencing peripheral sensitivity, spinal signaling, and descending pain modulation. Many people find it helps reduce pain sensitivity and improve recovery, especially when paired with movement-based rehab.
Is dry needling the same as acupuncture?
Dry needling is an acupuncture style because it uses the same solid filiform acupuncture needle. The difference is usually the clinical framework and treatment strategy: dry needling often focuses on myofascial trigger points and muscle-related pain patterns, while traditional acupuncture relies more on traditional acupoints and meridian-based point selection.
How many acupuncture or dry needling sessions do you need for chronic pain?
It depends on how long pain has been present and which mechanisms are driving symptoms. Chronic pain often improves with a series of treatments combined with progressive exercise and lifestyle factors (sleep, stress reduction, pacing). Many patients notice early changes in sensitivity within a few sessions, with longer-term improvements developing over weeks.
What’s the best treatment approach for chronic pain?
The best approach is usually individualized and multi-layered. Treatment often works best when it addresses peripheral drivers, nervous system sensitization, motor control changes, immune contributors, and psychosocial stressors. Needling-based therapies can be one useful tool within a broader plan.
Ready to Try Acupuncture & Dry Needling?
Whether you’re struggling with acute or chronic pain, acupuncture and dry needling may help restore mobility and reduce pain - quickly and safely.
📍 Conveniently located in New York City
🧠 Experts in trigger point therapy, acupuncture, and dry needling
Book your appointment today with the experts at Morningside Acupuncture, the top-rated acupuncture and dry needling clinic in New York City.
Let us help you move better, feel stronger, and live pain-free.
Additional Resources & Next Steps
Learn More: Visit our Blog for further insights into our treatment approach.
What to Expect: During your initial consultation, we perform a comprehensive evaluation to develop a personalized treatment plan.
Patient Stories: Read testimonials from patients who have experienced lasting relief.
Sources:
Lyndon, G. (2026). Pathophysiology of chronic pain: A mechanistic framework. Clinical Journal of Pain. https://pubmed.ncbi.nlm.nih.gov/41614224/
Disclaimer: This web site is intended for educational and informational purposes only. Reading this website does not constitute providing medical advice or any professional services. This information should not be used for diagnosing or treating any health issue or disease. Those seeking medical advice should consult with a licensed physician. Seek the advice of a medical doctor or other qualified health professional for any medical condition. If you think you have a medical emergency, call 911 or go to the emergency room. No acupuncturist-patient relationship is created by reading this website or using the information. Morningside Acupuncture PLLC and its employees and contributors do not make any express or implied representations with respect to the information on this site or its use. For any legal interpretation of scope of practice in your state, consult a licensed attorney or regulatory authority.
Read more from our blog