Understanding Incidental Shoulder MRI Findings
Infographic: You May Have a Rotator Cuff Tear or Shoulder Abnormality without Pain
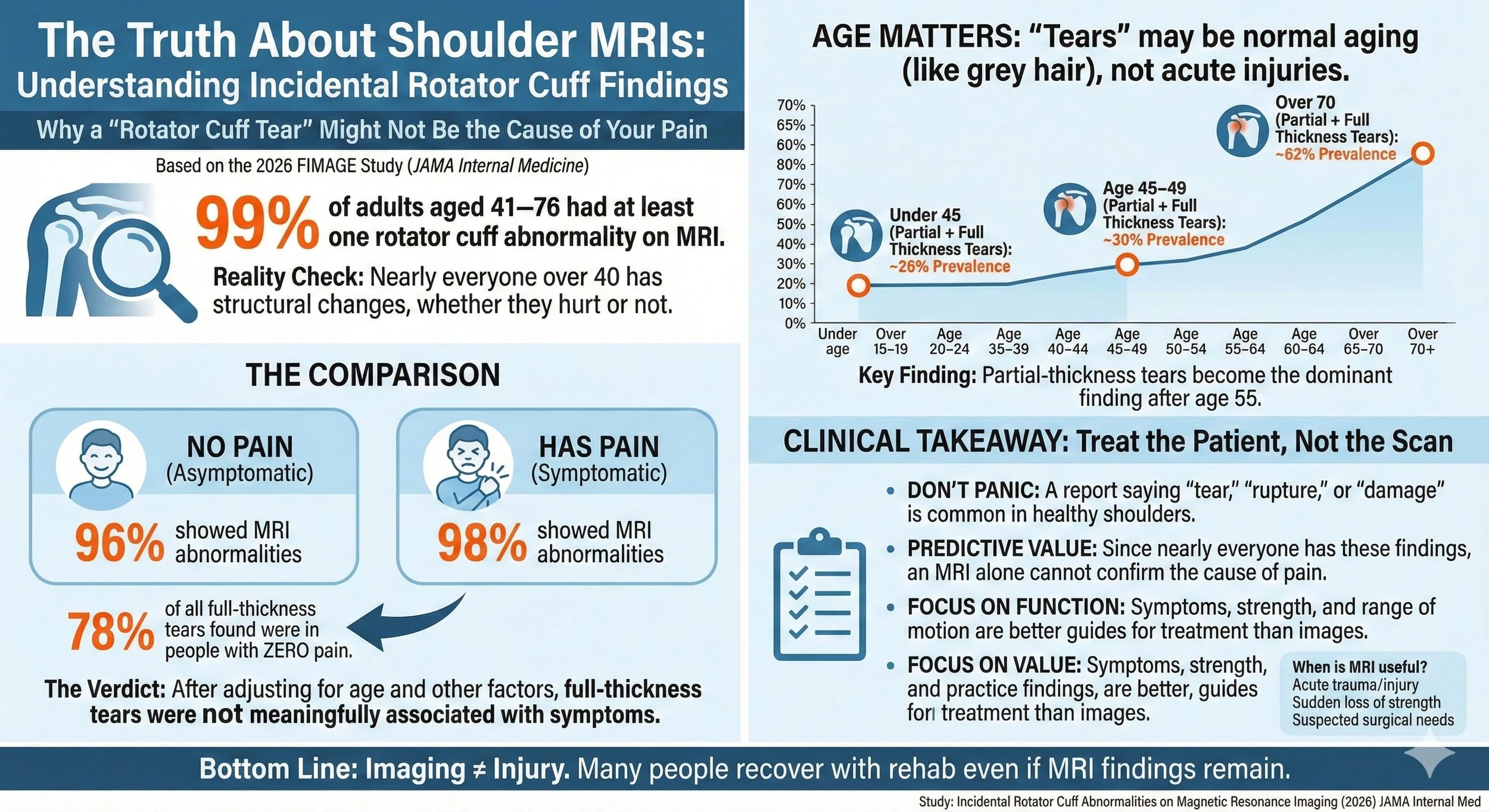
Most People Over 40 Have “Rotator Cuff Tears” on MRI Even Without Pain
What a new JAMA Internal Medicine study means for shoulder pain diagnosis
Shoulder pain is one of the most common musculoskeletal complaints in adults. Many patients are told they have a “rotator cuff tear” after an MRI. But how often do these imaging findings actually explain pain?
A large 2026 population-based study published in JAMA Internal Medicine provides one of the clearest answers we’ve seen so far and the results are striking.
Key Points
99% of adults aged 41–76 had at least one rotator cuff abnormality on MRI
96% of asymptomatic shoulders showed abnormalities
Even full-thickness tears were common in people without pain
After adjusting for clinical exam findings and other joint changes, full-thickness tears were not significantly associated with symptoms
Rotator cuff “abnormalities” appear to be largely age-related structural changes rather than reliable pain generators
Study Overview
This was the Finnish Imaging of Shoulder (FIMAGE) study, a nationally representative cross-sectional study conducted between 2023–2024 in Finland.
Participants
602 adults
Ages 41–76
Bilateral 3-Tesla MRI of both shoulders
Standardized clinical examination
Structured symptom assessment
Importantly, participants were recruited regardless of whether they had shoulder pain.
Only 18% reported current shoulder symptoms at the time of evaluation.
What Did the MRIs Show?
The findings were almost universal.
Overall Prevalence (Per Person)
That means 98.7% of participants had some form of rotator cuff abnormality.
Let that sink in.
Nearly everyone over 40 had structural changes.
Age Matters
The severity of findings increased with age:
No full-thickness tears under age 45
4% prevalence at ages 45–49
28–29% prevalence in those over 70
Partial-thickness tears became the dominant finding after age 55.
These changes appear to follow a degenerative pattern rather than an acute injury model.
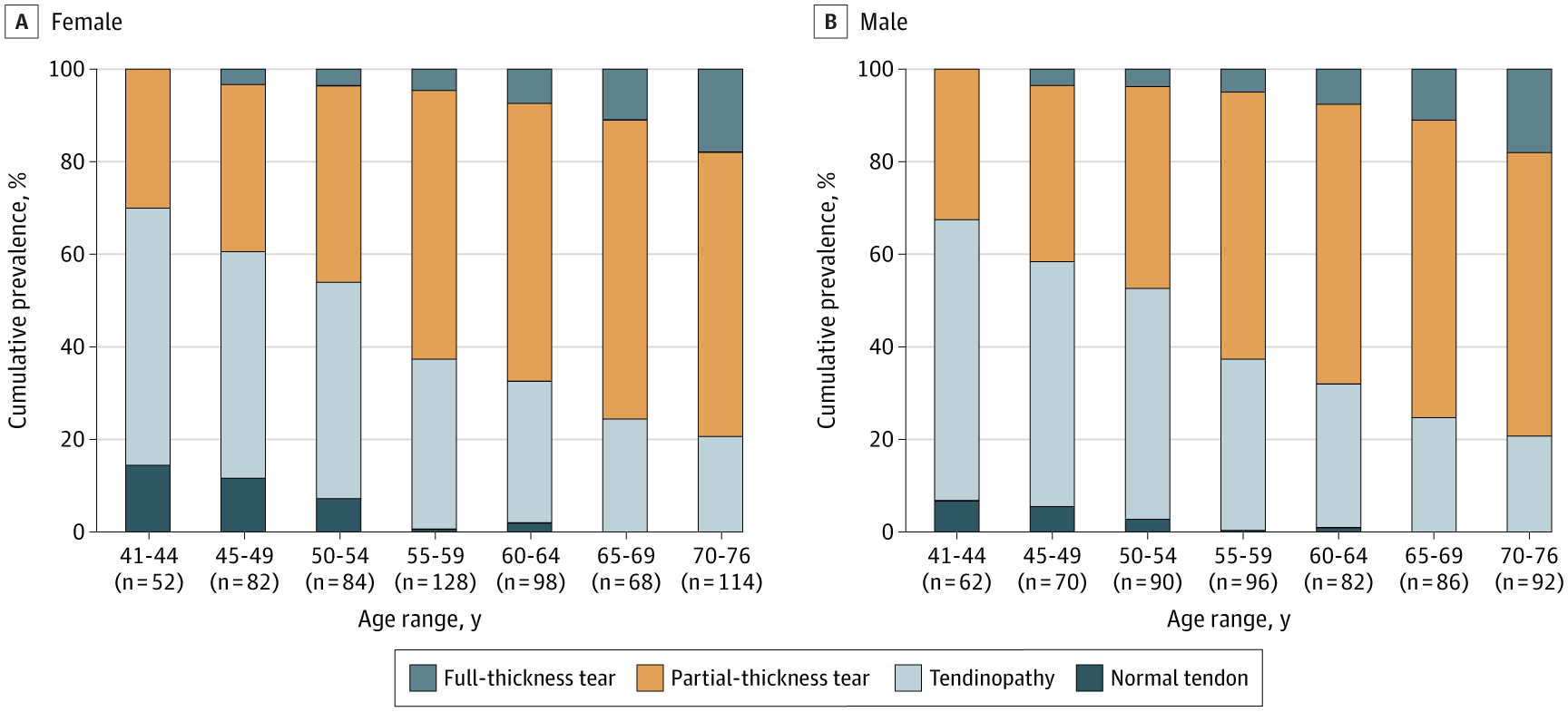
Figure from Ibounig et al., JAMA Internal Medicine, 2026. Licensed under CC-BY 4.0. DOI: 10.1001/jamainternmed.2025.7903.
The Most Important Question:
Do These MRI Findings Correlate With Pain?
This is where the study becomes clinically powerful.
Rotator Cuff Abnormalities by Shoulder (1,204 shoulders total):
At first glance, full-thickness tears seemed more common in symptomatic shoulders.
But after adjusting for:
Age
Sex
Education
Other MRI abnormalities (AC joint, GH joint, biceps)
Clinical exam findings
The difference disappeared.
The adjusted difference in full-thickness tear prevalence was:
0.8% (95% CI −3.4% to 6.0%).
In other words, once you account for other variables, full-thickness tears were not meaningfully associated with symptoms.
Even more striking:
Of the 96 full-thickness tears identified, 78% were in asymptomatic shoulders.
Why This Matters Clinically
This study challenges a deeply ingrained assumption:
“If the MRI shows a tear, that must be the cause of pain.”
But when nearly everyone over 50 has structural abnormalities, the positive predictive value of MRI findings drops dramatically.
The authors highlight an important diagnostic principle:
When the pretest probability of structural changes approaches 100%, the presence of those findings tells you very little about causality.
In simpler terms:
If almost everyone has it, it’s probably not the problem.
A Shift in Language: Are These Really “Tears”?
The authors suggest reconsidering terminology.
Words like:
Tear
Rupture
Damage
Carry emotional weight.
They imply something is broken and must be repaired.
But these findings may represent:
Age-related tendon remodeling
Degenerative fraying
Structural adaptation over time
This is similar to:
Meniscal “tears” in the knee
Disc “degeneration” in the spine
Both are extremely common in people without pain.
Implications for Imaging in Non-Traumatic Shoulder Pain
The study calls into question the routine use of MRI for non-traumatic shoulder pain.
MRI may still be appropriate when there is:
Acute trauma
Significant weakness
Progressive loss of function
Suspected surgical pathology
But for gradual, atraumatic shoulder pain, imaging findings alone appear insufficient to guide care.
What Does This Mean for Treatment?
This research reinforces a few important clinical principles:
1. Structural change ≠ pain
Pain is multifactorial and influenced by:
Local tissue sensitivity
Nervous system modulation
Movement patterns
Inflammation
Psychosocial context
2. Clinical examination matters more than imaging
History and functional testing remain critical.
3. Conservative care should often be first-line
Targeted strengthening
Neuromuscular retraining
Load management
Manual therapy
Needling-based interventions like acupuncture and dry needling
Surgery decisions should not rely on imaging alone.
How This Relates to Acupuncture and Dry Needling
When patients are told:
“You have a tear.”
Fear increases.
Movement decreases.
Guarding increases.
Pain often persists.
But if many of these findings represent normal age-related tendon changes, then treatment can focus on:
Modulating nociceptive input
Improving motor control
Reducing myofascial tension
Supporting graded loading
Acupuncture and dry needling (the use of a solid filiform acupuncture needle to interact with tissue and the nervous system) may help reduce local sensitivity and support neuromuscular adaptation within a comprehensive rehab plan.
This study reinforces that pain should be treated as a functional condition — not just a structural diagnosis.
Limitations of the Study
The authors note:
Population sample may not reflect severe specialty-care patients
Few very large tears in the cohort
Age range limited to 41–76
Conducted in Finland (limited ethnic diversity)
But the methodology was strong:
Blinded radiologists
High interobserver reliability
Bilateral imaging
Adjustment for confounders
This is currently one of the highest-quality prevalence studies on rotator cuff abnormalities.
Final Takeaway
Nearly every adult over 40 has rotator cuff abnormalities on MRI.
Most do not have pain.
Even full-thickness tears are often incidental.
This study strongly suggests that many rotator cuff findings represent age-related structural changes rather than definitive pain generators.
For clinicians and patients alike, the question should shift from:
“What does the MRI show?”
to:
“Does this finding actually explain the symptoms?”
That distinction can prevent unnecessary fear, overtreatment, and surgery.
Frequently Asked Questions (FAQ)
Can you have a rotator cuff tear and not know it?
Yes.
This study found that 96% of pain-free shoulders had rotator cuff abnormalities, including partial and full-thickness tears.
In fact, most full-thickness tears in the study were found in people without shoulder pain.
Many rotator cuff changes appear to be age-related structural changes rather than active injuries.
Does a rotator cuff tear always cause pain?
No.
The study showed very poor correlation between MRI findings and symptoms. After adjusting for other factors, even full-thickness tears were not clearly associated with shoulder pain.
Pain is influenced by many factors beyond structure, including:
Local inflammation
Nervous system sensitivity
Movement mechanics
Strength and load tolerance
If my MRI shows a rotator cuff tear, do I need surgery?
Not necessarily.
Many people improve with:
Progressive strengthening
Mobility work
Load management
Physical therapy
Needling-based treatments when appropriate
Surgery may be appropriate in cases involving:
Acute traumatic tears
Significant strength loss
Functional impairment
Failed conservative treatment
But imaging alone does not automatically mean surgery is required.
Do partial rotator cuff tears heal without surgery?
Partial-thickness tears often respond well to conservative care.
The body may not “heal” the tear in the sense of reversing it on imaging, but symptoms frequently improve through:
Tendon loading
Neuromuscular retraining
Reducing tissue irritability
Many structural changes remain visible on MRI even after symptoms resolve.
What is the difference between a partial and full-thickness rotator cuff tear?
A partial-thickness tear means part of the tendon is disrupted but not completely detached.
A full-thickness tear means the tendon is disrupted through its full depth.
However, this study showed that both types were common in people without pain.
Severity on imaging does not automatically predict symptom severity.
Should I get an MRI for shoulder pain?
It depends.
An MRI may be appropriate if you have:
A recent traumatic injury
Sudden loss of strength
Significant functional limitation
Surgical planning needs
For gradual, non-traumatic shoulder pain, early imaging may not change management and may lead to unnecessary worry.
Clinical evaluation and functional testing often provide more useful information initially.
Why do so many people have rotator cuff tears after age 40?
Rotator cuff tendons undergo age-related structural remodeling over time.
The study found:
62% had partial-thickness tears
11% had full-thickness tears
Prevalence increased steadily with age.
These changes appear to be part of normal aging rather than always representing acute injury.
Can I lift weights with a rotator cuff tear?
Often, yes — with appropriate programming.
Strength training is frequently part of rehabilitation for rotator cuff-related shoulder pain.
The key is:
Gradual loading
Proper mechanics
Symptom monitoring
Avoiding sudden overload
Many individuals continue athletic activity successfully despite imaging-confirmed tears.
Is my shoulder “damaged” if I have a tear on MRI?
Not necessarily.
Language like “tear” can imply something is broken.
But when nearly everyone over 50 has some degree of structural change, these findings may represent age-related adaptations rather than catastrophic damage.
The more important question is whether the finding explains your symptoms.
Why do doctors still order MRIs for shoulder pain?
Imaging is widely available and often expected by patients.
However, high-quality population data like this suggests that MRI findings must be interpreted carefully, especially in atraumatic shoulder pain
Ready to Try Acupuncture & Dry Needling?
Whether you’re struggling with acute or chronic pain, acupuncture and dry needling may help restore mobility and reduce pain - quickly and safely.
📍 Conveniently located in New York City
🧠 Experts in trigger point therapy, acupuncture, and dry needling
Book your appointment today with the experts at Morningside Acupuncture, the top-rated acupuncture and dry needling clinic in New York City.
Let us help you move better, feel stronger, and live pain-free.
Additional Resources & Next Steps
Learn More: Visit our Blog for further insights into our treatment approach.
What to Expect: During your initial consultation, we perform a comprehensive evaluation to develop a personalized treatment plan.
Patient Stories: Read testimonials from patients who have experienced lasting relief.
Sources:
Ibounig T, Järvinen TLN, Raatikainen S, Härkänen T, Sillanpää N, Bensch F, Haapamäki V, Toivonen P, Björkenheim R, Ryösä A, Kanto K, Lepola V, Joukainen A, Paavola M, Koskinen S, Rämö L, Buchbinder R, Taimela S. Incidental Rotator Cuff Abnormalities on Magnetic Resonance Imaging. JAMA Intern Med. 2026 Feb 16:e257903. doi: 10.1001/jamainternmed.2025.7903. PMID: 41697693; PMCID: PMC12910452. https://jamanetwork.com/journals/jamainternalmedicine/fullarticle/2844659
Disclaimer: This web site is intended for educational and informational purposes only. Reading this website does not constitute providing medical advice or any professional services. This information should not be used for diagnosing or treating any health issue or disease. Those seeking medical advice should consult with a licensed physician. Seek the advice of a medical doctor or other qualified health professional for any medical condition. If you think you have a medical emergency, call 911 or go to the emergency room. No acupuncturist-patient relationship is created by reading this website or using the information. Morningside Acupuncture PLLC and its employees and contributors do not make any express or implied representations with respect to the information on this site or its use. For any legal interpretation of scope of practice in your state, consult a licensed attorney or regulatory authority.
Read more from our blog