Acupuncture for Shoulder Bursitis
Subacromial Impingement, Rotator Cuff Trigger Points, and Why the Bursa Is Rarely the Original Problem
Shoulder bursitis is one of the most common shoulder diagnoses, yet the subacromial bursa seldom becomes inflamed on its own. Understanding what compresses it and what sensitizes the surrounding tissue points directly to why acupuncture and dry needling produce results that cortisone injections often cannot sustain.
- The subacromial bursa is the largest bursa in the body and sits between the rotator cuff tendons and the undersurface of the acromion; its primary function is to reduce friction during shoulder elevation, and it has no intrinsic role in shoulder stability or movement.
- Subacromial bursitis is almost always secondary to impingement; the bursa becomes compressed between the rotator cuff and the acromion when the subacromial space narrows, which can occur from acromial morphology (Type III hooked acromion) or, more commonly, from dynamic narrowing caused by rotator cuff muscle imbalance.
- Trigger points in the rotator cuff muscles, particularly the supraspinatus and infraspinatus, produce a local biochemical milieu that diffuses into the adjacent subacromial bursa, inducing secondary bursal inflammation without direct structural compression (Shah et al., 2008).
- The subscapularis is a frequently overlooked contributor; its trigger points create internal rotation bias that depresses the humeral head inferiorly and anteriorly, disrupting the precise centering of the humeral head under the acromion that prevents impingement.
- Acupuncture demonstrates clinically meaningful reductions in shoulder pain across multiple RCTs, with a large individual patient data meta-analysis finding significant superiority over both sham and no-treatment controls (Vickers et al., 2018).
- Cortisone injections into the subacromial bursa may reduce acute pain but do not address the muscle imbalance driving impingement; repeated injections carry risks of tendon weakening and, in some studies, accelerated rotator cuff degeneration (Coombes et al., 2010).
Shoulder Bursitis That Keeps Coming Back After Cortisone Injections?
Cortisone reduces bursal inflammation temporarily but cannot address the rotator cuff trigger points and muscle imbalances that created the impingement in the first place. At Morningside, we target the supraspinatus, infraspinatus, and subscapularis directly, restoring the muscle balance that keeps the humeral head centered under the acromion and the subacromial space open. Schedule to assess what is driving your shoulder bursitis pattern.
Schedule NowThe Subacromial Space: A Tight Corridor That Tolerates Little Disruption
The subacromial space is the gap between the superior surface of the rotator cuff tendons and the inferior surface of the acromion, the coracoacromial ligament, and the acromioclavicular joint. In an average adult, this space measures roughly 9 to 10 millimeters at rest. The subacromial bursa and the supraspinatus tendon both pass through this corridor, which means there is almost no tolerance for anything that reduces its height.
The acromion's shape is one structural variable that affects this space. Bigliani and colleagues classified acromial morphology into three types: Type I (flat undersurface), Type II (curved), and Type III (hooked). A hooked Type III acromion reduces the subacromial space at the anterior margin and is associated with higher rates of rotator cuff pathology. However, acromial morphology is a fixed anatomical feature; it does not explain why bursitis develops, resolves with treatment, and recurs months later. That pattern points to dynamic factors in the surrounding musculature rather than to bone shape alone.
Related Muscles That Cause Shoulder PainDynamic Narrowing: How Muscle Imbalance Compresses the Bursa
The humeral head's position within the glenoid fossa during shoulder movement is not passive; it depends on the coordinated action of the rotator cuff muscles to keep it centered. During arm elevation, the supraspinatus, infraspinatus, teres minor, and subscapularis work together to compress the humeral head into the glenoid while the deltoid produces the upward force of elevation. If the rotator cuff's centering force is reduced relative to the deltoid's superior pull, the humeral head migrates superiorly into the subacromial space and compresses whatever is there, including the bursa and the supraspinatus tendon.
Trigger points are a primary mechanism of this imbalance. A muscle harboring active trigger points generates less force at its normal resting length because the taut band containing the trigger point is already at near-maximum mechanical tension; it has reduced capacity for voluntary contraction. When the supraspinatus, infraspinatus, or subscapularis develop trigger points, their centering force decreases, and the humeral head rides higher during elevation. This is dynamic narrowing: the subacromial space is anatomically normal, but the muscle imbalance creates intermittent compression with every arm elevation cycle (Simons et al., 1999).
The Rotator Cuff Trigger Point Contribution
Beyond the mechanical impingement that trigger points produce through muscle inhibition, there is a direct chemical mechanism connecting trigger points to bursal inflammation. Research examining the biochemical environment at trigger point sites has found elevated concentrations of substance P, calcitonin gene-related peptide, bradykinin, serotonin, and inflammatory cytokines in the immediate tissue surrounding an active trigger point (Shah et al., 2008). These substances diffuse into adjacent structures, and given the proximity of the supraspinatus and infraspinatus to the subacromial bursa, the bursa is directly exposed to this inflammatory milieu.
This means that even when subacromial space dimensions are adequate, trigger points in the rotator cuff can induce bursal inflammation through chemical diffusion, independent of mechanical compression. This is a clinically important point because it explains why some patients with normal subacromial space measurements on imaging still develop and maintain bursitis, and why dry needling the rotator cuff directly can reduce bursal inflammation without ever entering the bursa itself.
| Muscle | Role in Bursitis | Trigger Point Referral | Treatment Priority |
|---|---|---|---|
| Supraspinatus | Initiates shoulder abduction and compresses the humeral head into the glenoid; trigger points reduce its centering force and allow superior humeral migration; adjacent to the bursa, directly bathing it in inflammatory biochemicals | Deep lateral shoulder pain; mid-deltoid aching; lateral epicondyle region | Highest priority; supraspinatus trigger points are among the most consistent findings in subacromial bursitis |
| Infraspinatus | External rotator; trigger points refer pain anteriorly to the shoulder and down the arm; inhibition allows anterior humeral head drift and increases anterior impingement | Anterior shoulder pain; deep shoulder joint; lateral arm and forearm; may refer to the hand | Very high priority; infraspinatus is one of the most commonly affected muscles in shoulder pain syndromes and has a large referred pain territory |
| Subscapularis | Internal rotator; trigger points bias the shoulder into internal rotation, which anteriorizes the humeral head and reduces posterior cuff effectiveness; frequently missed because it is not accessible without specific positioning | Posterior shoulder (between scapula and rib cage); wrist band distribution; axilla | High priority and frequently overlooked; shoulder bursitis that does not fully respond to treatment of the external rotators often has a subscapularis component |
| Deltoid | Powerful arm elevator; when the rotator cuff's centering force is insufficient, the deltoid's superior pull dominates and drives the humeral head into the subacromial space during arm elevation | Local deltoid aching; lateral shoulder; difficulty sleeping on the affected side | Secondary target; addressing the rotator cuff imbalance usually corrects the deltoid's excessive superior pull, but active deltoid trigger points may also require direct treatment |
| Teres Minor | External rotator that works in parallel with the infraspinatus; trigger points contribute to reduced posterior cuff force and anterior shoulder instability | Small, focused posterior deltoid region; lateral shoulder button | Moderate priority; typically addressed alongside infraspinatus as part of the posterior cuff complex |
| Coracobrachialis | Anterior shoulder muscle attached to the coracoid process; trigger points contribute to anterior shoulder tightness and limit full external rotation, increasing impingement with overhead activities | Anterior shoulder; posterior arm; dorsal forearm and hand (referred distally) | Lower priority; typically treated after the rotator cuff complex has been addressed, if anterior shoulder tightness persists |
Distinguishing Bursitis from Calcific Tendinitis and Rotator Cuff Tear
Three shoulder conditions often share a clinical picture of anterolateral shoulder pain with painful arc on elevation, and distinguishing them changes the treatment approach meaningfully. Subacromial bursitis, calcific tendinitis, and partial or full-thickness rotator cuff tears can coexist or be easily confused based on symptoms alone.
Calcific tendinitis involves calcium hydroxyapatite crystal deposition within the rotator cuff tendon itself, most commonly the supraspinatus. During the resorptive phase, when the body is dissolving the calcium deposit, the resulting inflammatory cascade is among the most acutely painful events in musculoskeletal medicine; patients often report sudden, severe pain that makes the shoulder nearly unusable. Ultrasound or plain radiography identifies the calcific deposit, distinguishing it from uncomplicated bursitis. Acupuncture may reduce the pain associated with calcific tendinitis, particularly during subacute and chronic phases, but needling into an active resorptive calcific deposit warrants caution.
Rotator cuff tears present a different consideration. Partial-thickness tears may have a pain pattern nearly identical to bursitis, and they frequently coexist with bursitis. Full-thickness tears with significant weakness, particularly weakness in external rotation or abduction, benefit from orthopedic evaluation. Acupuncture and dry needling can reduce pain in patients with partial rotator cuff tears by addressing the surrounding trigger points and secondary muscle guarding, but treatment goals differ from bursitis without structural tear. An MRI is the definitive test when tear is suspected.
Not Sure Whether Your Shoulder Pain Is Bursitis, a Rotator Cuff Issue, or Something Else?
At Morningside, the initial assessment includes a thorough shoulder evaluation to identify which tissues are contributing to your pain, whether there are active trigger points in the rotator cuff, and whether your pain pattern suggests a structural issue that warrants imaging. We work with what is treatable and refer when structural evaluation changes the picture. Schedule a new patient appointment to get clarity on what is actually driving your shoulder pain.
Schedule NowWhat Acupuncture and Dry Needling Address in Shoulder Bursitis
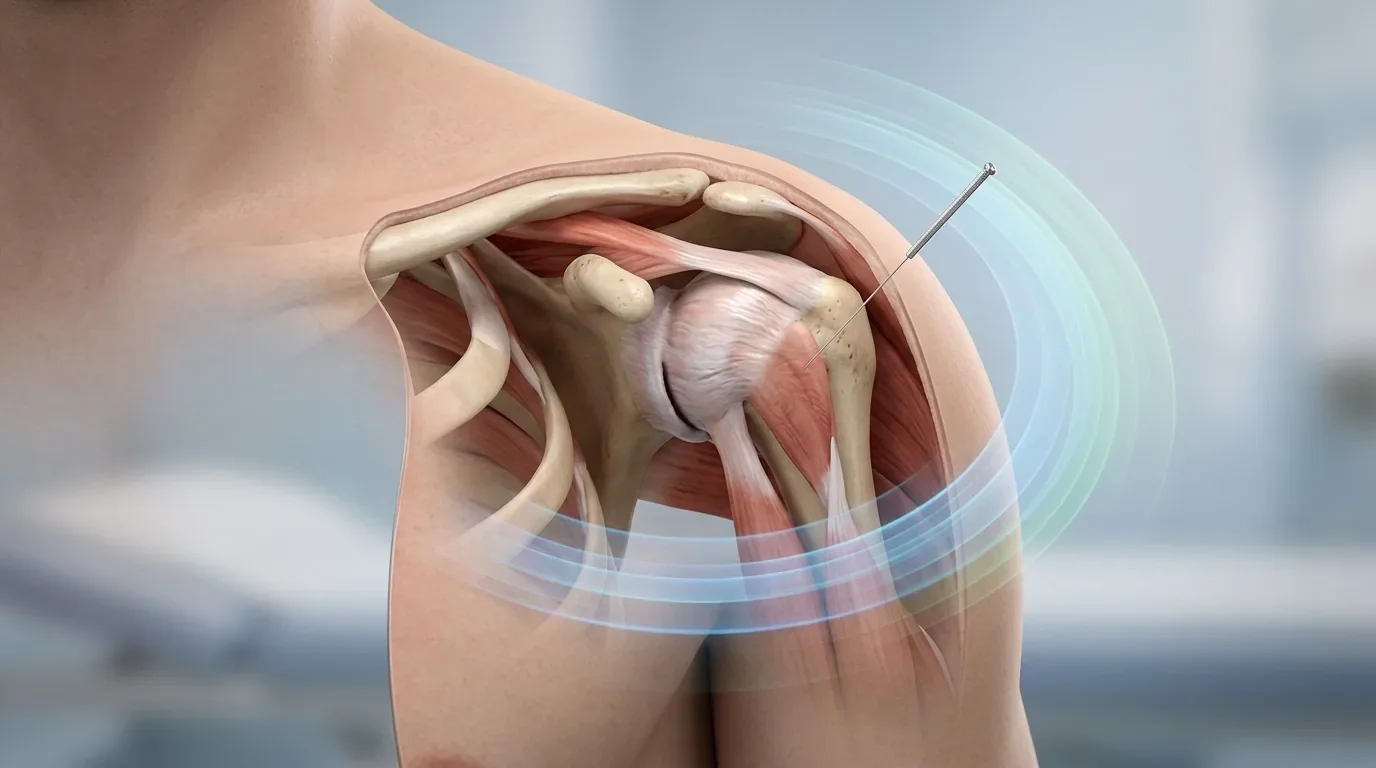
The treatment logic follows directly from the anatomy. Dry needling the supraspinatus, infraspinatus, teres minor, and subscapularis trigger points addresses the impingement mechanism at its source. Resolving these trigger points restores the rotator cuff's centering force, reduces the frequency and magnitude of humeral head migration during elevation, and removes the chemical inflammatory burden that the trigger points were diffusing into the adjacent bursa. The bursa does not need to be injected to reduce its inflammation if the source of that inflammation is removed upstream.
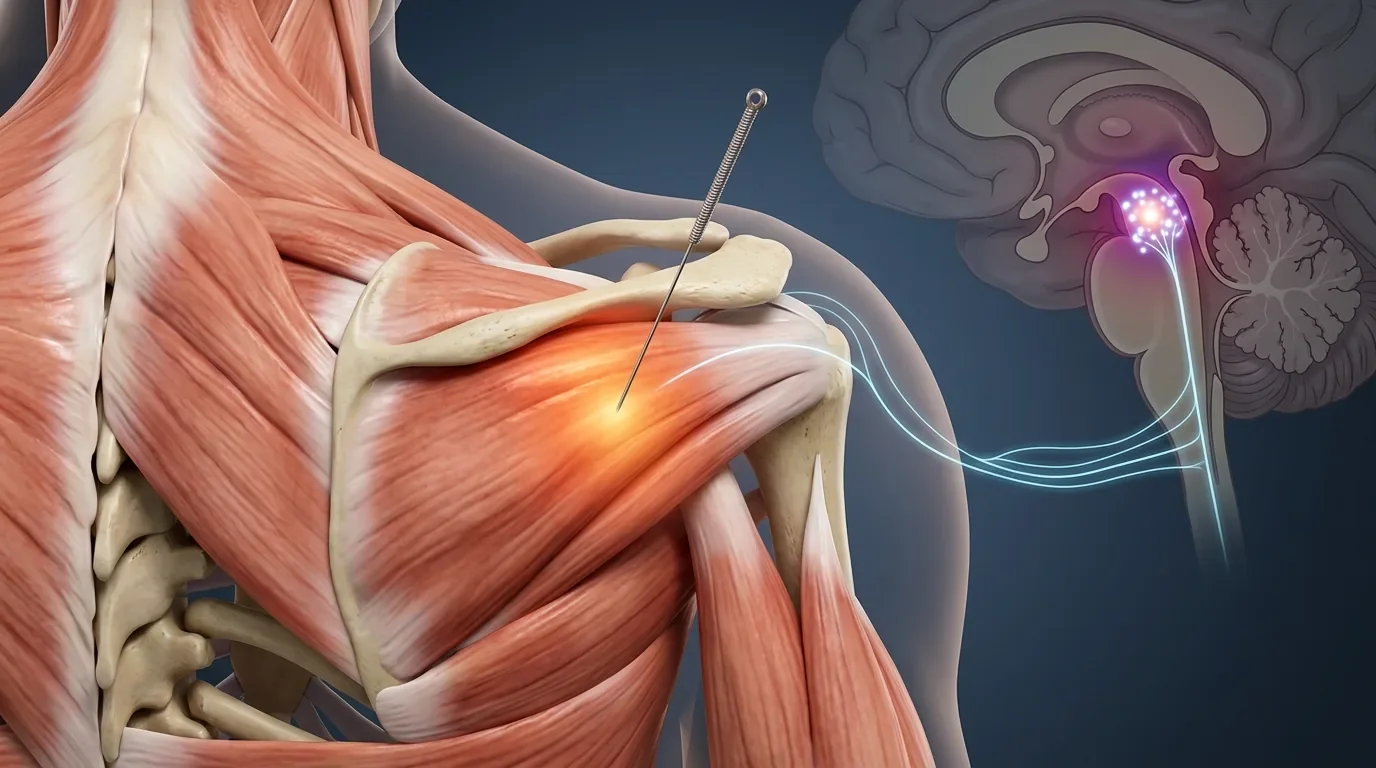
Traditional acupuncture complements dry needling through the descending inhibitory system. Needle stimulation activates periaqueductal gray matter projections through the raphe nuclei, releasing serotonin and norepinephrine onto dorsal horn interneurons and attenuating the central sensitization component of shoulder pain (Zhao, 2008). Patients with long-standing shoulder bursitis frequently have significant central sensitization, where pain responses are amplified beyond what the local tissue state warrants; acupuncture's central effects address this component in a way that local injection cannot.
Periosteal needling, placing the needle tip against the acromion, coracoid process, or greater tuberosity, activates local mechanoreceptors and has documented effects on localized periosteal tenderness. This technique is useful when the patient has developed secondary tenderness at the bony margins of the subacromial space.
Related Dry Needling for Shoulder Pain Related Trigger Points Treatment at MorningsideA Note on Cortisone Injections
Subacromial cortisone injections can provide meaningful short-term pain relief, and for patients in acute flares they remain a reasonable option. The limitations become apparent over time. Corticosteroid injections into tendinous tissue carry risks of tendon weakening; systematic reviews have found that early pain relief from cortisone injections is frequently followed by outcomes inferior to physical therapy or no-treatment controls at 6 to 12 months (Coombes et al., 2010). Repeated injections amplify these concerns, as glucocorticoids inhibit collagen synthesis and may accelerate the tissue degeneration they were intended to palliate.
For the typical patient with recurrent shoulder bursitis driven by rotator cuff trigger points and muscle imbalance, cortisone reduces the symptom without addressing its cause. Combining a cortisone injection with dry needling of the rotator cuff muscles in the days following an injection, when the acute pain is reduced enough to permit comfortable tissue access, can leverage the injection's short-term benefit while addressing the longer-term drivers. This combined approach is used selectively at Morningside for patients who arrive mid-flare and cannot tolerate direct tissue work at presentation.
Shoulder Bursitis Treatment in New York City
At Morningside Acupuncture, we are the highest-rated acupuncture and dry needling clinic in New York City with over 500 five-star Google reviews. We treat shoulder bursitis by working directly on the rotator cuff trigger points that produce impingement, combining dry needling for the local tissue drivers with traditional acupuncture for the central sensitization component. Whether your shoulder pain is a recent first episode or a years-long pattern of flares and partial remissions, we can assess what is driving it and build a plan that addresses more than the inflammation. Schedule your new patient appointment today.
Schedule NowFrequently Asked Questions
What does shoulder bursitis feel like?
Shoulder bursitis typically produces a deep, aching pain in the lateral shoulder that worsens with arm elevation, particularly in the arc between 60 and 120 degrees (the "painful arc"). Reaching overhead, across the body, or behind the back is painful. Lying on the affected shoulder at night is often the most consistent complaint, as the pressure of lying compresses the already-sensitized subacromial space. Acute bursitis may produce swelling and warmth at the lateral shoulder, while chronic bursitis tends toward a duller, more diffuse aching without visible swelling.
Does shoulder bursitis go away on its own?
Mild acute bursitis from a single overuse event often resolves with relative rest and anti-inflammatory measures over several weeks. Chronic or recurrent bursitis, which is the pattern most patients present with, does not reliably resolve without addressing the underlying rotator cuff trigger points and muscle imbalances that are driving the impingement. If the bursa is being compressed with every arm elevation cycle because the humeral head is not centering properly, rest provides temporary relief but the bursitis returns as soon as full activity resumes.
Is dry needling painful for shoulder bursitis?
Direct dry needling of the supraspinatus, infraspinatus, and subscapularis produces the characteristic "twitch response" and a brief muscle cramping sensation as the trigger point is deactivated. Most patients describe this as a few seconds of intense but tolerable discomfort, followed by a release and often immediate reduction in shoulder heaviness. The subscapularis requires positioning the shoulder in external rotation to access the anterior surface of the scapula; this is more complex than superficial muscles but well within normal practice when performed by a trained practitioner. Post-treatment soreness for 24-48 hours is common, similar to delayed onset muscle soreness after exercise.
How many sessions does it take to see improvement in shoulder bursitis?
Many patients notice meaningful changes within 3 to 5 sessions, though the timeline depends on how long the bursitis has been present and how much central sensitization has developed. Recent-onset bursitis with identifiable rotator cuff trigger points and no significant structural damage often responds quickly. Long-standing bursitis with years of compensatory movement patterns, secondary cervical involvement, and central sensitization may require more sessions to fully address all contributing factors. A reasonable expectation is significant improvement in daily pain and overhead function within 6 to 8 sessions.
Can Morningside treat shoulder bursitis if I have also been told I have a rotator cuff tear?
Yes, and in fact the combination is common. Partial rotator cuff tears frequently coexist with subacromial bursitis, and the surrounding trigger points in intact rotator cuff fibers and in adjacent muscles like the infraspinatus and teres minor contribute substantially to the pain even when a tear is present. Dry needling the intact portions of the rotator cuff, reducing secondary muscle guarding, and addressing central sensitization can meaningfully reduce pain in patients with partial tears. Full-thickness tears with functional weakness affecting daily activities benefit from orthopedic evaluation to discuss whether surgical repair is appropriate, and we are happy to co-manage alongside surgical care when needed.
References
- Vickers, A. J., Vertosick, E. A., Lewith, G., MacPherson, H., Foster, N. E., Sherman, K. J., Irnich, D., Witt, C. M., & Linde, K. (2018). Acupuncture for chronic pain: Update of an individual patient data meta-analysis. Journal of Pain, 19(5), 455-474. https://doi.org/10.1016/j.jpain.2017.11.005
- Simons, D. G., Travell, J. G., & Simons, L. S. (1999). Travell & Simons' Myofascial Pain and Dysfunction: The Trigger Point Manual (2nd ed.). Williams & Wilkins.
- Shah, J. P., Danoff, J. V., Desai, M. J., Parikh, S., Nakamura, L. Y., Phillips, T. M., & Gerber, L. H. (2008). Biochemicals associated with pain and inflammation are elevated in sites near to and remote from active myofascial trigger points. Archives of Physical Medicine and Rehabilitation, 89(1), 16-23. https://doi.org/10.1016/j.apmr.2007.10.018
- Coombes, B. K., Bisset, L., & Vicenzino, B. (2010). Efficacy and safety of corticosteroid injections and other injections for management of tendinopathy: a systematic review of randomised controlled trials. The Lancet, 376(9754), 1751-1767.
- Zhao, Z. Q. (2008). Neural mechanism underlying acupuncture analgesia. Progress in Neurobiology, 85(4), 355-375. https://doi.org/10.1016/j.pneurobio.2008.05.004
- Kietrys, D. M., Palombaro, K. M., Azzaretto, E., Hubler, R., Schaller, B., Schlussel, J. M., & Tucker, M. (2013). Effectiveness of dry needling for upper-quarter myofascial pain: A systematic review and meta-analysis. Journal of Orthopaedic & Sports Physical Therapy, 43(9), 620-634. https://doi.org/10.2519/jospt.2013.4668
Disclaimer: This web site is intended for educational and informational purposes only. Reading this website does not constitute providing medical advice or any professional services. This information should not be used for diagnosing or treating any health issue or disease. Those seeking medical advice should consult with a licensed physician. Seek the advice of a medical doctor or other qualified health professional for any medical condition. If you think you have a medical emergency, call 911 or go to the emergency room. No acupuncturist-patient relationship is created by reading this website or using the information. Morningside Acupuncture PLLC and its employees and contributors do not make any express or implied representations with respect to the information on this site or its use. For any legal interpretation of scope of practice in your state, consult a licensed attorney or regulatory authority.
Read more from our blog