Acupuncture for Rotator Cuff Pain
How Dry Needling and Acupuncture Address the Myofascial, Inflammatory, and Neurological Components of Rotator Cuff Injuries
Rotator cuff pain is one of the most common presentations at Morningside Acupuncture, and it is also one of the most treatable with needling. Understanding why requires looking beyond the structural tear itself to the myofascial trigger points, central sensitization, and altered shoulder mechanics that are often the primary sources of persistent pain and limitation.
- Myofascial trigger points in the rotator cuff muscles and surrounding shoulder musculature are frequently the dominant pain generators in rotator cuff patients, contributing pain and movement limitation independently of any structural tear; dry needling these trigger points often produces significant and lasting relief.
- The infraspinatus muscle contains trigger points that refer pain to the front of the shoulder and outer upper arm, precisely mimicking the location and quality of pain reported by many patients diagnosed with supraspinatus tendinopathy or impingement; this pattern is so common it has been called one of the most frequently missed shoulder diagnoses.
- Subscapularis trigger points refer pain to the posterior shoulder, upper arm, and wrist, and produce a characteristic limitation in shoulder external rotation that can mimic adhesive capsulitis (frozen shoulder); deactivating these trigger points can restore range of motion quickly and dramatically.
- A 10-year randomized controlled trial by Moosmayer and colleagues (2019) found no significant difference in outcomes between surgical rotator cuff repair and structured conservative exercise therapy for small-to-medium tears, reinforcing that conservative management including acupuncture and dry needling is the evidence-based first-line approach for most patients.
- Acupuncture activates descending pain inhibitory pathways from the periaqueductal gray and raphe nuclei, reducing central sensitization that amplifies shoulder pain signals beyond what the structural findings would predict (Zhao, 2008); this is particularly relevant for patients whose pain seems disproportionate to imaging findings.
- The combination of dry needling for myofascial trigger points and traditional acupuncture for systemic pain modulation, guided by findings from the individual patient assessment, provides a comprehensive approach that addresses the full pain mechanism rather than targeting imaging findings alone (Vickers et al., 2018).
Has Your Shoulder Pain Persisted Despite Injections or Physical Therapy?
At Morningside Acupuncture, we assess both the structural components and the myofascial trigger point patterns that contribute to rotator cuff pain. Many patients find that the majority of their shoulder pain resolves through dry needling of the infraspinatus and subscapularis, even when imaging shows a structural tear.
Schedule NowWhy Rotator Cuff Pain Is Not Simply About the Tear
The diagnosis of "rotator cuff tear" tends to focus clinical attention on the structural finding visible on MRI and to frame the pain in terms of that finding. This framing misses several important clinical realities. First, population-based MRI studies have consistently shown that rotator cuff tears are extremely common in asymptomatic adults, present in roughly 30 percent of people over 60 and over 50 percent of those over 70. A tear on MRI is not, by itself, a sufficient explanation for pain. Second, the muscles that form the rotator cuff develop myofascial trigger points in response to overuse, trauma, and altered biomechanics, and these trigger points produce referred pain patterns that are often indistinguishable from tendon-origin pain. Third, persistent shoulder pain sensitizes the central nervous system, amplifying pain signals in ways that persist even after tissue healing has occurred. An effective treatment approach needs to address all three of these dimensions.
The Myofascial Dimension: Which Muscles Refer Where
The four rotator cuff muscles, together with the surrounding shoulder girdle musculature, produce referred pain patterns that account for a substantial portion of what patients experience as "shoulder pain." Understanding these patterns is essential to targeted dry needling treatment.
Infraspinatus
The infraspinatus sits on the posterior surface of the scapula and is responsible for external rotation and horizontal abduction of the shoulder. Its trigger points refer pain anteriorly to the front of the shoulder, the outer arm, and sometimes down the outer forearm and into the hand. This anterior referral pattern is precisely where most patients localize their shoulder pain, which is why infraspinatus trigger points are so frequently mistaken for supraspinatus tendinopathy, biceps tendinitis, or impingement. Patients often report that they cannot reach behind their back or sleep on the affected shoulder, both of which are consistent with infraspinatus involvement.
Supraspinatus
The supraspinatus sits above the scapular spine in the supraspinous fossa and initiates the first 15 to 20 degrees of shoulder abduction. Its trigger points refer a deep aching pain to the outer shoulder and upper arm, and a secondary reference zone reaches down the outer forearm to the wrist. Supraspinatus trigger points are associated with a characteristic painful arc during shoulder abduction, typically occurring in the 60 to 120 degree range, which overlaps exactly with the painful arc attributed to subacromial impingement.
Subscapularis
The subscapularis occupies the anterior surface of the scapula and is the primary internal rotator of the shoulder. Its trigger points produce one of the most clinically dramatic referral patterns in the shoulder: deep posterior shoulder pain, upper arm pain, and a distinctive band of referred pain around the wrist. The subscapularis also produces limitation in external rotation that can be so severe that patients are diagnosed with adhesive capsulitis. Unlike true frozen shoulder, however, subscapularis trigger point-related restriction can often be substantially relieved within a single treatment session of dry needling, providing a useful diagnostic distinction.
Teres Minor
The teres minor, located along the axillary border of the scapula, assists infraspinatus in external rotation. Its trigger points refer pain to the posterior deltoid region and outer arm, and uniquely among the rotator cuff muscles, they frequently cause numbness and tingling in the fourth and fifth fingers that can be mistaken for cubital tunnel syndrome or C8 radiculopathy.
| Muscle | Primary Referral Zone | Common Misdiagnosis | Key Clinical Clue |
|---|---|---|---|
| Infraspinatus | Anterior shoulder, outer arm, outer forearm | Supraspinatus tendinopathy, biceps tendinitis, impingement | Pain at front of shoulder despite muscle being at back; can't sleep on side |
| Supraspinatus | Outer shoulder, upper arm, outer forearm to wrist | Subacromial impingement, AC joint pain | Painful arc 60-120 degrees; deep aching rather than sharp pain |
| Subscapularis | Posterior shoulder, upper arm, wrist band | Adhesive capsulitis, posterior shoulder pain | Restricted external rotation; wrist pain with no wrist pathology |
| Teres minor | Posterior deltoid, outer arm, ring and little finger | Cubital tunnel syndrome, C8 radiculopathy | Finger numbness reproduced by pressure on posterior axillary border |
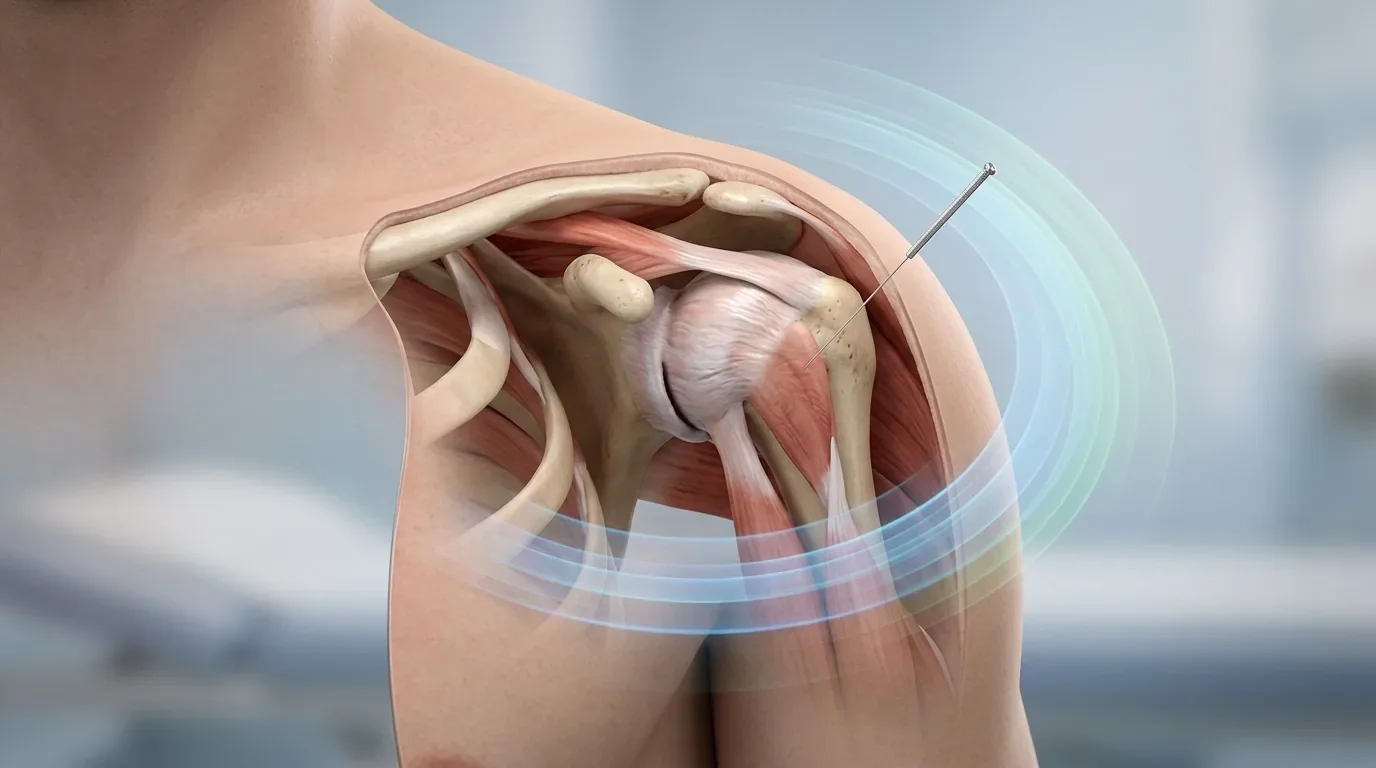
How Dry Needling Addresses Rotator Cuff Pain
Dry needling targets the myofascial trigger points within the rotator cuff muscles and the broader shoulder girdle musculature. The needle is inserted directly into the palpable taut band containing the trigger point. In many cases this elicits a local twitch response, a brief involuntary contraction of the muscle fibers within the taut band, which is associated with the release of the trigger point and normalization of the local biochemical environment. Studies examining the biochemistry of active trigger points find elevated concentrations of substance P, calcitonin gene-related peptide, bradykinin, and inflammatory cytokines; these levels normalize after effective treatment (Shah et al., 2008).
For the rotator cuff specifically, needling the infraspinatus and subscapularis frequently produces the most immediate pain relief because these muscles are so commonly the primary generators of the anterior and posterior shoulder pain patients describe. The supraspinatus, teres minor, and surrounding muscles including the deltoid, pectoralis minor, biceps, and the muscles attaching to the medial scapular border are systematically assessed and needled based on individual findings.
Accessing the Subscapularis
The subscapularis occupies the anterior surface of the scapula and is less accessible than the posterior rotator cuff muscles. Practitioners trained in dry needling reach it by positioning the arm in abduction, locating the lateral border of the scapula through the axilla, and directing the needle along the costal surface of the scapula. This is a technique-sensitive approach that requires significant training and anatomical familiarity, and it produces striking results when subscapularis trigger points are the source of the patient's pain and restricted external rotation.
Ready to Find Out If Trigger Points Are Driving Your Shoulder Pain?
At Morningside Acupuncture, every shoulder patient receives a myofascial assessment of the full rotator cuff and surrounding musculature as part of the initial intake. Many patients who have been managing rotator cuff pain for months or years find substantial relief through targeted dry needling within the first few sessions.
Schedule NowAcupuncture for Central Pain Modulation
Beyond the local effects of dry needling on trigger points, traditional acupuncture needle stimulation activates central nervous system pain inhibitory pathways that are clinically relevant for rotator cuff patients, particularly those with persistent or widespread shoulder pain that seems disproportionate to imaging findings.
Acupuncture needle stimulation of A-delta and C-fiber afferents produces signals that travel to the periaqueductal gray (PAG) in the midbrain, which in turn activates the rostral ventromedial medulla (RVM) and initiates descending inhibition of nociceptive signals at the dorsal horn of the spinal cord (Zhao, 2008). This descending inhibitory cascade involves the release of endogenous opioids (enkephalin, beta-endorphin, dynorphin), serotonin, and norepinephrine, all of which reduce the gain on pain transmission. For patients with central sensitization, where the nervous system has become hyperreactive and amplifies normal shoulder sensory signals into severe pain, this central modulation is often as important as the local trigger point treatment.
The individual patient data meta-analysis by Vickers and colleagues (2018), which pooled data from 39 high-quality trials involving nearly 21,000 patients, found that acupuncture produced meaningful reductions in shoulder and neck pain that persisted at 12-month follow-up, with effect sizes well above the threshold considered clinically important. This positions acupuncture as a durable treatment rather than a temporary symptomatic fix.
Acupuncture After Rotator Cuff Surgery
For patients who have undergone surgical repair of the rotator cuff, acupuncture and dry needling serve as valuable adjuncts to post-operative rehabilitation. Surgery addresses the structural pathology but does not resolve the myofascial trigger points that developed in the surrounding musculature before and during the period of shoulder dysfunction. These trigger points persist after surgery and contribute to post-operative pain and stiffness.
Post-operative dry needling in the weeks following surgery, once the surgical site has sufficiently healed and the treating physiotherapist or surgeon has cleared soft tissue work, can reduce post-operative pain, improve range of motion recovery, and allow more effective engagement with the exercise rehabilitation that is the primary determinant of surgical outcome. Traditional acupuncture simultaneously addresses post-operative pain through central inhibitory pathways and supports the inflammatory resolution that is part of tissue healing.
| Phase | Primary Goals | Acupuncture / Dry Needling Role | Typical Frequency |
|---|---|---|---|
| Acute (0-6 weeks) | Pain control; protect healing tissue; maintain gentle movement | Systemic acupuncture for pain modulation; needling of non-irritated surrounding muscles | 1-2x per week |
| Subacute (6-12 weeks) | Restore range of motion; begin progressive loading; address trigger points | Dry needling of rotator cuff and scapular stabilizer trigger points; full myofascial assessment | 1x per week |
| Rehabilitation (3-6 months) | Rebuild strength and endurance; restore sport/work capacity | Dry needling to address limiting trigger points; acupuncture for central sensitization if present | Every 2-4 weeks as needed |
| Post-surgical (as applicable) | Reduce post-operative pain; support ROM recovery; enable effective PT engagement | Gentle surrounding muscle needling once cleared; progressive inclusion of repaired area | 1-2x per week during active rehab |
| Maintenance | Prevent recurrence; manage occupational or activity-related flares | Periodic dry needling of high-load muscles; acupuncture for pain flares | Monthly or as needed |
What to Expect at Morningside Acupuncture
Initial appointments for rotator cuff pain at Morningside Acupuncture begin with a comprehensive intake that includes the patient's history of the shoulder problem, any imaging findings, previous treatments and their responses, and the patient's current functional limitations and goals. The physical assessment examines active and passive range of motion, identifies the pattern of painful movements and positions, and systematically palpates each of the rotator cuff muscles and surrounding shoulder girdle musculature for trigger points and taut bands.
Treatment typically combines dry needling of the identified trigger points with traditional acupuncture points selected for their systemic pain modulatory effects. Patients with rotator cuff pain often notice meaningful improvement within two to four sessions, though the complete course of treatment depends on the severity of trigger point involvement, the presence or absence of a structural tear, and how much central sensitization has developed. Most patients with isolated myofascial shoulder pain complete a course of 6 to 10 sessions; those with larger structural tears or longer pain histories may require longer courses with periodic maintenance sessions thereafter.
Start Your Shoulder Recovery at New York City's Highest-Rated Acupuncture Clinic
Morningside Acupuncture is the highest-rated acupuncture and dry needling clinic in New York City with over 500 five-star Google reviews. Our practitioners specialize in the precise myofascial assessment and dry needling techniques that address the full range of contributors to rotator cuff pain, from the trigger points that refer to the front of the shoulder to the central sensitization that keeps pain alive long after tissue injury has resolved.
Schedule NowFrequently Asked Questions
Can acupuncture help a rotator cuff tear heal faster?
Acupuncture and dry needling do not directly repair torn tendon tissue, but they address the pain, muscle dysfunction, and limited range of motion that prevent effective rehabilitation. By deactivating the trigger points that contribute to pain and movement limitation, and by supporting the anti-inflammatory environment through cholinergic and neuroimmune mechanisms, acupuncture enables patients to engage more fully with the strengthening exercises that are the primary driver of recovery from small and medium rotator cuff tears.
How many sessions are typically needed for rotator cuff pain?
Most patients with rotator cuff pain notice meaningful improvement within two to four sessions. A complete initial course typically involves 6 to 10 sessions over 4 to 8 weeks, depending on severity, pain duration, and whether a structural tear is present. Patients with longer-standing pain or significant central sensitization may require more sessions. After the initial course, periodic maintenance treatments every four to eight weeks help prevent recurrence, particularly for patients with physically demanding occupations or sports that load the shoulder regularly.
My MRI shows a full thickness tear. Is acupuncture still appropriate?
Yes, in most cases. The 10-year randomized controlled trial by Moosmayer and colleagues (2019) found that structured conservative management produced outcomes equivalent to surgical repair for small and medium full-thickness tears. Acupuncture and dry needling are valuable components of conservative management, addressing the myofascial trigger points and central sensitization that contribute substantially to pain and disability regardless of the structural finding. For large or complete tears in younger, active patients, surgical consultation is appropriate, and acupuncture can still play a supportive role in the post-operative rehabilitation period.
I have been told my shoulder pain is from impingement, not a tear. Can acupuncture help?
Shoulder impingement syndrome is strongly associated with myofascial trigger points in the supraspinatus and infraspinatus that reproduce the painful arc during arm elevation. Dry needling of these muscles, along with the periscapular stabilizers that influence how the scapula positions during arm movement, frequently resolves impingement-related pain. Acupuncture is well-supported for shoulder pain more broadly, and many patients diagnosed with impingement find that their symptoms resolve completely with trigger point dry needling without the need for corticosteroid injections or surgery.
Is it safe to receive acupuncture right after a rotator cuff injury?
Acupuncture is generally safe in the early stages following a rotator cuff injury. Treatment in the acute phase focuses on systemic pain modulation and needling of muscles away from the acutely inflamed area rather than directly at the injury site. As the acute phase resolves, typically within two to six weeks, more direct dry needling of the rotator cuff muscles becomes appropriate. Any patient who has undergone surgery should wait for clearance from their surgeon or physical therapist before beginning dry needling of the surgical area.
References
- Moosmayer, S., Lund, G., Seljom, U. S., Haldorsen, B., Svege, I. C., Hennig, T., Pripp, A. H., & Smith, H. J. (2019). At a 10-year follow-up, tendon repair is superior to physiotherapy in the treatment of small and medium-sized rotator cuff tears. Journal of Bone and Joint Surgery, 101(12), 1050-1060. https://doi.org/10.2106/JBJS.18.01373
- Simons, D. G., Travell, J. G., & Simons, L. S. (1999). Travell and Simons' Myofascial Pain and Dysfunction: The Trigger Point Manual (2nd ed., Vol. 1). Lippincott Williams & Wilkins.
- Zhao, Z. Q. (2008). Neural mechanism underlying acupuncture analgesia. Progress in Neurobiology, 85(4), 355-375. https://doi.org/10.1016/j.pneurobio.2008.05.004
- Vickers, A. J., Vertosick, E. A., Lewith, G., MacPherson, H., Foster, N. E., Sherman, K. J., Irnich, D., Witt, C. M., & Linde, K. (2018). Acupuncture for chronic pain: Update of an individual patient data meta-analysis. Journal of Pain, 19(5), 455-474. https://doi.org/10.1016/j.jpain.2017.11.005
- Shah, J. P., Danoff, J. V., Desai, M. J., Parikh, S., Nakamura, L. Y., Phillips, T. M., & Gerber, L. H. (2008). Biochemicals associated with pain and inflammation are elevated in sites near to and remote from active myofascial trigger points. Archives of Physical Medicine and Rehabilitation, 89(1), 16-23. https://doi.org/10.1016/j.apmr.2007.10.018
- Kietrys, D. M., Palombaro, K. M., Azzaretto, E., Huber, R., Schaller, B., Schlussel, J. M., & Tucker, M. (2013). Effectiveness of dry needling for upper-quarter myofascial pain: A systematic review and meta-analysis. Journal of Orthopaedic & Sports Physical Therapy, 43(9), 620-634. https://doi.org/10.2519/jospt.2013.4668
Disclaimer: This web site is intended for educational and informational purposes only. Reading this website does not constitute providing medical advice or any professional services. This information should not be used for diagnosing or treating any health issue or disease. Those seeking medical advice should consult with a licensed physician. Seek the advice of a medical doctor or other qualified health professional for any medical condition. If you think you have a medical emergency, call 911 or go to the emergency room. No acupuncturist-patient relationship is created by reading this website or using the information. Morningside Acupuncture PLLC and its employees and contributors do not make any express or implied representations with respect to the information on this site or its use. For any legal interpretation of scope of practice in your state, consult a licensed attorney or regulatory authority.
Read more from our blog