Dry Needling for Shoulder Pain

Dry needling for shoulder pain
Reaching overhead to grab a plate sparks a sharp pinch at the top of the arm; by evening, crossing the chest to fasten a seatbelt feels tight and sore. That pattern is common in non-traumatic shoulder pain. Many presentations include a musculoskeletal cue—rotator-cuff guarding, scapular muscle tension, or pectoral tightness—before or during a flare. While shoulder pain is multifactorial, trigger points in rotator-cuff and shoulder-girdle muscles can add mechanical input to an already irritated system.
Dry needling for shoulder pain addresses this mechanical component. The approach targets muscles known to refer pain to the deltoid region, lateral arm, or top of the shoulder. When the picture includes pinching with overhead reach, end-range guarding, or a familiar band of ache at the upper arm, reducing trigger-point irritability may lower overall nociceptive input and help decrease symptom intensity or frequency.
Background on technique and what sessions involve is outlined in the Dry Needling Guide, and pain-referral maps appear in the Trigger Points Guide.
Key Points
Most suitable cases: shoulder pain patterns with muscular cues—pinch or “catch” with overhead reach, post-workout soreness that lingers, or scapular fatigue with desk work.
Primary effect: reduction of trigger-point activity in rotator-cuff and shoulder-girdle muscles that commonly refer pain to the deltoid, lateral arm, and acromial region.
Muscle coverage: a shoulder-relevant set is assessed; treatment selection is based on the individual’s referral pattern and findings.
Expected timeline: noticeable change is often reported within 1–3 sessions; a short series of approximately 4–6 visits is common. Chronic patterns may require 10 or more visits or ongoing care.
Practical trial: 3–5 sessions (adjusted if responses are delayed or highly variable).
Session pacing: dosing is conservative and progressed according to comfort and symptom changes between visits.
Shoulder Pain: Brief Condition Overview
Shoulder pain often fluctuates with elevation, loading, and posture. Many presentations include a muscular component that contributes to symptom severity, particularly at end-range reach or with repetitive activity.
Signs & symptoms (common features):
Pain with motion/load: painful arc during elevation, reaching behind the back, or horizontal adduction; possible night discomfort when lying on the shoulder.
Stiffness/guarding: palpable taut bands in rotator-cuff or periscapular muscles; reduced tolerance to overhead or behind-the-back tasks.
Localized referral: ache over the deltoid, lateral arm, or superior shoulder; sometimes a line of pain toward the bicipital groove.
Musculoskeletal cues: postural fatigue, scapular dyskinesia, pectoral/chest tightness, or “pull” at the posterior shoulder with cross-body reach.
Typical triggers: repetitive overhead work or sport, deconditioning, rapid load spikes, prolonged mouse/keyboard tasks, and sleep posture.
Typical treatment (commonly used approaches):
Acute strategies: time-limited analgesics as appropriate, relative rest, graded exposure to reach, and modification of provocative tasks.
Preventive options: clinician-guided exercise progression and load management tailored to goals and tolerance.
Lifestyle & behavioral support: regular sleep/wake times, hydration, pacing/graded activity, position changes during desk work.
Rehab and bodywork (when musculoskeletal drivers are present): dry needling, manual therapy, and targeted exercise to reduce rotator-cuff/periscapular muscle irritability and improve shoulder/scapular coordination.
Shoulder Pain Trigger Points Summary
Front of shoulder pain
- Deltoid Primary
- Biceps Brachii Secondary
- Pectoralis Major Secondary
- Subclavius Secondary
- Supraspinatus Secondary
- Subscapularis Secondary
- Coracobrachialis Secondary
Back of shoulder pain
- Deltoid Primary
- Levator Scapulae Primary
- Supraspinatus Secondary
- Teres Major Secondary
- Teres Minor Secondary
- Subscapularis Secondary
- Pectoralis Minor Secondary
- Infraspinatus Secondary
Back of arm pain
- Scalene Primary
- Teres Major Primary
- Triceps Brachii Secondary
- Deltoid Secondary
- Subscapularis Secondary
- Supraspinatus Secondary
- Teres Minor Secondary
- Latissimus Dorsi Secondary
- Serratus Posterior Superior Secondary
- Coracobrachialis Secondary
Front of arm pain
- Pectoralis Major Primary
- Deltoid Secondary
- Subscapularis Secondary
- Supraspinatus Secondary
- Infraspinatus Secondary
- Scalene Secondary
Upper thoracic back pain
- Scalene Primary
- Levator Scapulae Primary
- Trapezius Primary
- Multifidi Primary
- Supraspinatus Secondary
- Rhomboid Secondary
- Splenius Cervicis Secondary
- Triceps Brachii Secondary
- Biceps Brachii Secondary
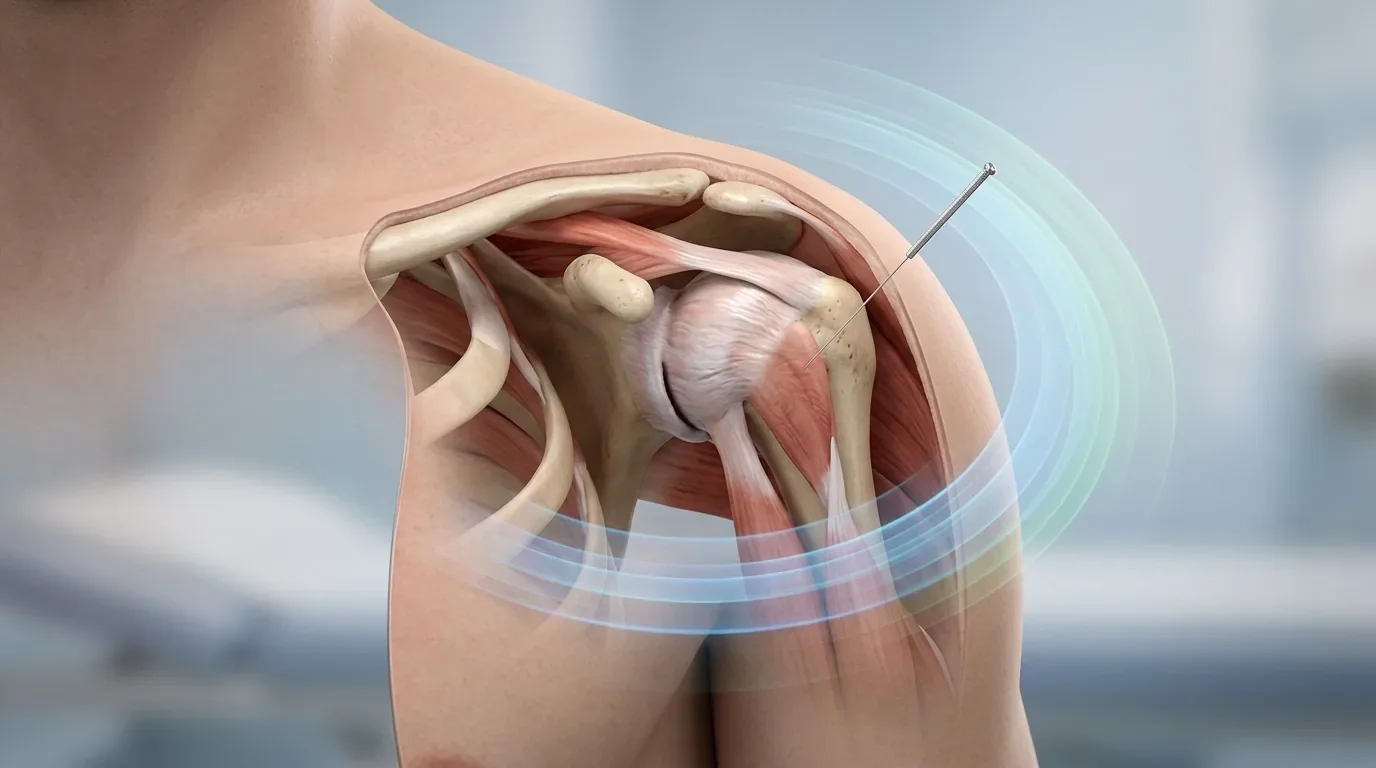
How Dry Needling Fits Shoulder Pain with Rotator-Cuff/Scapular Triggers
Dry needling is best considered when flares reliably coincide with musculoskeletal drivers: a pinch at mid-arc elevation, posterior shoulder “pull” during cross-body reach, or scapular fatigue after desk work. In such cases, hyper-irritable trigger points can refer pain to the deltoid region and lateral arm, sustaining a feedback loop of guarding and limited motion.
Treatment uses a thin, solid filiform needle to stimulate targeted neuromuscular tissue. A brief dull ache, localized twitch, or familiar spread toward the deltoid or lateral arm is common during needling and indicates accurate targeting. While a single tight muscle is not responsible for all shoulder pain, addressing muscular input can be materially helpful when rotator-cuff or periscapular tension is part of the pattern. Additional technique context is provided in the Dry Needling Guide.
Shoulder Pain Referral Patterns and Associated Trigger Points
This section outlines common shoulder pain patterns linked to specific muscles, identified through detailed symptom mapping. Understanding these muscle involvement patterns helps guide precise palpation and treatment tailored to the individual's unique referral pain. The following list categorizes muscles by common pain locations to assist in targeted assessment and intervention.
Front of shoulder pain
Deltoid (Primary): The deltoid can generate front of shoulder aching when trigger points refer pain to the anterior deltoid insertion.
Biceps Brachii (Secondary): Biceps brachii trigger points commonly produce pain at the front of the shoulder due to referral to the bicipital groove region.
Pectoralis Major (Secondary): Pectoralis major trigger points are known to project pain to the anterior shoulder, mimicking rotator cuff issues.
Subclavius (Secondary): Subclavius can contribute to front-of-shoulder pain by referring discomfort toward the clavicle and anterior deltoid.
Supraspinatus (Secondary): Supraspinatus referral patterns often target the lateral and anterior upper arm, resulting in apparent front-shoulder pain.
Subscapularis (Secondary): Subscapularis trigger points may refer pain to the front of the shoulder and down the upper arm, leading to persistent aches.
Coracobrachialis (Secondary): This muscle can cause symptoms at the front of the shoulder due to referral to the anterior deltoid and upper arm.
Back of shoulder pain
Deltoid (Primary): Posterior deltoid trigger points refer pain directly to the back of the shoulder, often mimicking rotator cuff injury.
Levator Scapulae (Primary): Levator scapulae refers pain to the upper shoulder blade and neck, which may present as deep back-of-shoulder discomfort.
Supraspinatus (Secondary): The supraspinatus may refer pain to the posterior aspect of the shoulder and lateral arm.
Teres Major (Secondary): Teres major referral patterns often produce aching along the posterior shoulder and down the arm.
Teres Minor (Secondary): Teres minor trigger points can mimic deep back-of-shoulder pain and radiate toward the arm.
Subscapularis (Secondary): Subscapularis may present with pain in the posterior shoulder due to its broad referral zone.
Pectoralis Minor (Secondary): Pectoralis minor referrals can extend to the back of the shoulder and upper arm, especially with postural strain.
Infraspinatus (Secondary): Infraspinatus frequently refers deep aching to the posterior shoulder and upper arm.
Back of arm pain
Scalene (Primary): Scalene trigger points can refer pain down the posterior arm, sometimes causing numbness or tingling.
Teres Major (Primary): Teres major can be a source of pain in the back of the arm due to its referral into the triceps region.
Triceps Brachii (Secondary): Triceps brachii trigger points often cause aching along the length of the posterior upper arm.
Deltoid (Secondary): Deltoid trigger points may result in pain radiating into the back of the arm, especially with overhead activity.
Subscapularis (Secondary): Subscapularis referral can extend along the upper and posterior arm, presenting as diffuse discomfort.
Supraspinatus (Secondary): Supraspinatus can cause pain in the back of the arm through referral to the lateral and posterior deltoid.
Teres Minor (Secondary): Teres minor trigger points may generate posterior arm pain that worsens with rotation or reach.
Latissimus Dorsi (Secondary): Latissimus dorsi referral commonly affects the posterior upper arm, especially with pulling or lifting.
Serratus Posterior Superior (Secondary): Serratus posterior superior can refer sharp pain toward the posterior aspect of the upper arm.
Coracobrachialis (Secondary): Coracobrachialis may present with pain radiating down the back of the arm due to its referral pattern.
Front of arm pain
Pectoralis Major (Primary): Pectoralis major trigger points frequently refer discomfort along the front of the arm and chest.
Deltoid (Secondary): Anterior deltoid trigger points often extend pain down the front of the arm, especially with repetitive lifting.
Subscapularis (Secondary): Subscapularis may produce pain that travels along the inside of the arm toward the wrist.
Supraspinatus (Secondary): Supraspinatus referral patterns can create pain over the front of the shoulder and arm.
Infraspinatus (Secondary): Infraspinatus can generate front-of-arm pain by referring deeply to the anterior humerus.
Scalene (Secondary): Scalene trigger points may shoot pain down the front of the arm, contributing to forearm and hand symptoms.
Upper thoracic back pain
Scalene (Primary): Scalenes may cause upper thoracic back discomfort as their referral targets the upper back and interscapular region.
Levator Scapulae (Primary): Levator scapulae trigger points frequently refer pain to the upper thoracic back and medial scapula border.
Trapezius (Primary): Trapezius referral commonly spans the upper back and neck, causing widespread thoracic tightness.
Multifidi (Primary): Multifidus trigger points create localized pain in the thoracic spine, especially after prolonged sitting or twisting.
Supraspinatus (Secondary): Supraspinatus referrals may reach the upper back and acromial region, mimicking thoracic pain.
Rhomboid (Secondary): Rhomboid trigger points produce aching between the shoulder blades, common in upper thoracic complaints.
Splenius Cervicis (Secondary): Splenius cervicis can refer pain into the upper thoracic spine and posterior neck.
Triceps Brachii (Secondary): Triceps brachii referral occasionally presents with discomfort radiating to the upper thoracic back and scapular area.
Biceps Brachii (Secondary): Biceps brachii may mimic upper thoracic pain through referral zones that cross the shoulder and upper back.
What to Expect in a Session (Comfort, Pacing, Soreness)
A typical visit begins with a concise review of symptom frequency/pattern, triggers, activity and position tolerance, and any warning signs that a flare is beginning. Glenohumeral and scapulothoracic motion are checked, followed by targeted palpation to identify taut bands and reproduction of familiar referral. The examination informs which muscles are addressed first and how many sites are suitable for the initial appointment.
During needling, a spreading ache or brief twitch may be noticed; these responses tend to settle within seconds. Sessions are focused on symptoms with gradual progression over time.
Post-session soreness commonly feels workout-like and can last 24–72 hours. Simple after-care—hydration and comfortable shoulder/scapular mobility—usually keeps this predictable and brief. An overview of session flow and common responses appears in the Dry Needling Guide.
Relief Timeline & Visit Cadence
Early change—such as reduced painful arc, less end-range guarding, or easier overhead reach—is often reported within 1–3 sessions. To influence overall frequency or intensity, a short series of approximately 4–6 sessions is common. Chronic patterns, particularly with long-standing muscular contributors or frequent flares, may require 10 or more visits or ongoing care at a lower maintenance frequency. Spacing is adjusted to sensitivity and schedule (weekly or slightly longer intervals are typical).
Progress is tracked against meaningful markers: number of “bad days,” reliance on short-term relief, or post-flare recovery time. If these metrics are unchanged after a 3–5 session practical trial, treatment variables are adjusted (e.g., alternate muscle priorities, dosing, or visit spacing) or further evaluation is considered.
Dry Needling for Shoulder Pain Research
Dry Needling of Rotator Cuff Trigger Points for Chronic Shoulder Pain (2025)
A randomized controlled trial found that deep dry needling of rotator cuff trigger points significantly improves pain, functional disability, grip strength, and shoulder stability in patients with chronic rotator cuff–related shoulder pain. Improvements exceeded minimal clinically important differences and were sustained at a one-week follow-up. Clinicians should consider incorporating dry needling into rehabilitation protocols for shoulder pain as this study demonstrates clinically meaningful benefits in stability and pain reduction—see protocol details and outcomes in this trial of dry needling for rotator cuff–related shoulder pain.
Analgesic Effects of Dry Needling in Shoulder Myofascial Pain Syndrome (2021)
This randomized, sham-controlled study showed that a single session of trigger point dry needling produced significant pain relief and reduction in mechanical hyperalgesia area in patients with chronic shoulder myofascial pain syndrome; effects persisted for at least a week. Participants experienced improvements in pain intensity and pain interference with daily activity beginning two days after intervention. For further details, clinical implications, and discussion of mechanistic insights, refer to dry needling analgesic effect in shoulder pain.
Dry Needling Improves Pain in Hemiparetic Shoulder After Stroke (2020)
A double-blind, crossover randomized trial examined dry needling applied to trigger points versus non-trigger point areas in post-stroke patients with hemiparetic shoulder pain. Dry needling at trigger points resulted in a more substantial decrease in shoulder pain scores at two- and four-week follow-ups, compared to non-trigger point needling. This highlights the importance of targeted trigger point dry needling as an effective intervention for persistent shoulder pain with post-stroke muscle involvement—see protocol and follow-up details in dry needling for post-stroke hemiparetic shoulder pain.
Frequently Asked Questions (FAQ)
Can dry needling help with shoulder pain?
It can be helpful when a muscle-driven component is evident—e.g., consistent rotator-cuff or periscapular tension that precedes or accompanies flares and is reproducible on examination. In such cases, reducing trigger-point activity may lower the mechanical input that aggravates symptoms.
How many sessions are needed before results are clear?
A practical trial is 3–5 sessions. Some individuals notice change sooner, while others require a short series to shift frequency or intensity. If progress is not observable in tracked metrics, treatment variables are revised accordingly.
Ready to Try Acupuncture & Dry Needling?
Whether you’re struggling with acute or chronic pain, acupuncture and dry needling may help restore mobility and reduce pain - quickly and safely.
📍 Conveniently located in New York City
🧠 Experts in trigger point therapy, acupuncture, and dry needling
Book your appointment today with the experts at Morningside Acupuncture, the top-rated acupuncture and dry needling clinic in New York City.
Let us help you move better, feel stronger, and live pain-free.
Additional Resources & Next Steps
Learn More: Visit our Blog for further insights into our treatment approach.
What to Expect: During your initial consultation, we perform a comprehensive evaluation to develop a personalized treatment plan.
Patient Stories: Read testimonials from patients who have experienced lasting relief.
Sources:
Moosavi, S., Lajevardi, L., Mehravar, M., & Bagheri, S. (2025). The effect of rotator cuff trigger points dry needling on the stability, pain, grip strength, and disability in patients with chronic rotator cuff-related shoulder pain: A randomized controlled trial. Journal of Shoulder and Elbow Surgery, 34(6), 1219-1230. https://pubmed.ncbi.nlm.nih.gov/40537393/
Barreto, S. S., Gurgel, R. K., & Franco, A. (2021). Dry needling has lasting analgesic effect in shoulder pain. Pain Reports, 6(3), e8240781. https://pmc.ncbi.nlm.nih.gov/articles/PMC8240781/
Calvo-Lobo, C., et al. (2020). Changes in Muscle Tone, Function, and Pain in the Hemiparetic Shoulder After Dry Needling: A Controlled Randomized Crossover Trial. Journal of Manipulative and Physiological Therapeutics, 43(9), 870-878. https://pubmed.ncbi.nlm.nih.gov/32488238/
Disclaimer: This web site is intended for educational and informational purposes only. Reading this website does not constitute providing medical advice or any professional services. This information should not be used for diagnosing or treating any health issue or disease. Those seeking medical advice should consult with a licensed physician. Seek the advice of a medical doctor or other qualified health professional for any medical condition. If you think you have a medical emergency, call 911 or go to the emergency room. No acupuncturist-patient relationship is created by reading this website or using the information. Morningside Acupuncture PLLC and its employees and contributors do not make any express or implied representations with respect to the information on this site or its use.
Read more from our blog