Dry Needling for Back Pain

Dry needling for back pain
“After a full day at the laptop, a line of tightness forms above the belt; by evening, bending forward is a chore.”
That pattern is common in non-specific low back pain. Many presentations include a musculoskeletal cue—quadratus lumborum tightness, paraspinal guarding, or hip-stabilizer referral—before or during a flare.
While back pain is multifactorial, trigger points in the spinal and hip muscles can add mechanical input to an already irritated system.
Dry needling for back pain addresses this mechanical component. The approach targets muscles known to refer pain to the lumbosacral region, buttock, and posterior hip. When the picture includes stiffness, protective bracing, or familiar bands of ache, reducing trigger-point irritability may lower overall nociceptive input and help decrease symptom intensity or frequency.
Background on technique and what sessions involve is outlined in the Dry Needling Guide, and pain-referral maps appear in the Trigger Points Guide.
For readers interested in evidence, see:
Key Points
Most suitable cases: back pain patterns with clear muscular cues—morning stiffness that eases with movement, end-of-day paraspinal tightness, or buttock referral after sitting.
Primary effect: reduction of trigger-point activity in lumbar paraspinals and hip stabilizers that commonly refer pain to the low back and buttock.
Muscle coverage: a back-pain–relevant set is assessed; treatment selection is based on the individual’s referral pattern and findings.
Expected timeline: noticeable change is often reported within 1–3 sessions; a short series of approximately 4–6 visits is common. Chronic patterns may require 10 or more visits or ongoing care.
Practical trial: 3–5 sessions (adjusted if responses are delayed or highly variable).
Session pacing: dosing is conservative and progressed according to comfort and symptom changes between visits.
Back Pain: Brief Condition Overview
Back pain involves recurrent or persistent pain between the lower ribs and gluteal folds, often fluctuating with position, load, and activity. Many presentations include a muscular component that contributes to symptom severity during flares.
Signs & symptoms (common features):
Pain with position: worse after prolonged sitting/standing; may ease with gentle movement.
Stiffness/guarding: palpable taut bands in paraspinals or hip stabilizers; reduced flexion/rotation tolerance.
Buttock or posterior hip ache: may accompany lumbar pain without clear radicular signs.
Musculoskeletal cues: “belt-line” tightness, QL tenderness, paraspinal knots, or gluteal referral after walking or sitting.
Typical triggers: deconditioning, sudden load spikes, prolonged static posture, sleep disruption, stress, or repetitive bending.
Typical treatment (commonly used approaches):
Acute strategies: time-limited analgesics as appropriate, relative rest, graded movement, and activity modification at flare onset.
Preventive options: clinician-guided strategies, exercise progression, and load management tailored to goals and tolerance.
Lifestyle & behavioral support: regular sleep/wake times, hydration, pacing/graded activity, stress management.
Rehab and bodywork (when musculoskeletal drivers are present): dry needling, manual therapy, and targeted exercise to reduce lumbar/hip muscle irritability and improve movement tolerance.
Back Pain Trigger Points
Quadratus lumborum (QL)
Why it’s important: Common in “belt-line” ache and side-bending restrictions; often overworks with prolonged sitting/standing or asymmetric loads.
Referral pain zone: Ipsilateral low back, iliac crest region, and superior gluteal area.
Multifidus
Why it’s important: Segmental stabilizer that guards with repeated flexion/extension and postural fatigue; a frequent source of focal stiffness.
Referral pain zone: Deep, localized lumbar ache adjacent to the spinous column.
Iliocostalis lumborum & Iliocostalis thoracis
Why they’re important: Key erector-spinae components that flare with prolonged posture, deconditioning, or sudden load spikes.
Referral pain zone: Longitudinal bands along the lumbar/thoracolumbar column; may echo into upper buttock or posterior ribs.
Erector spinae (thoracolumbar)
Why it’s important: Global extensor group often presenting as palpable “cords” and end-of-day tightness after desk or lifting work.
Referral pain zone: Broad paraspinal strip with possible wrap to posterior rib angles.
Gluteus medius
Why it’s important: Lateral hip stabilizer that compensates for pelvic control deficits; often irritated by prolonged standing/walking.
Referral pain zone: Posterolateral hip and upper buttock; can mimic “sciatic-like” ache without true radicular signs.
Gluteus minimus
Why it’s important: Deep stabilizer that overloads with prolonged sitting or gait asymmetries; a frequent driver of referred buttock ache.
Referral pain zone: Lateral/posterior hip and buttock; may project down the lateral thigh in select patterns.
Piriformis
Why it’s important: Deep external rotator sensitive to prolonged sitting or rapid training changes; interacts with pelvic mechanics.
Referral pain zone: Deep central buttock; may extend toward the posterior thigh in certain presentations.
Psoas major
Why it’s important: Hip flexor that contributes to a “compressed” lumbar feel with prolonged sitting or repetitive flexion/lifting.
Referral pain zone: Anterior hip/groin with secondary perception of lumbar tightness.
How Dry Needling Fits Back Pain with Lumbar/Hip Triggers
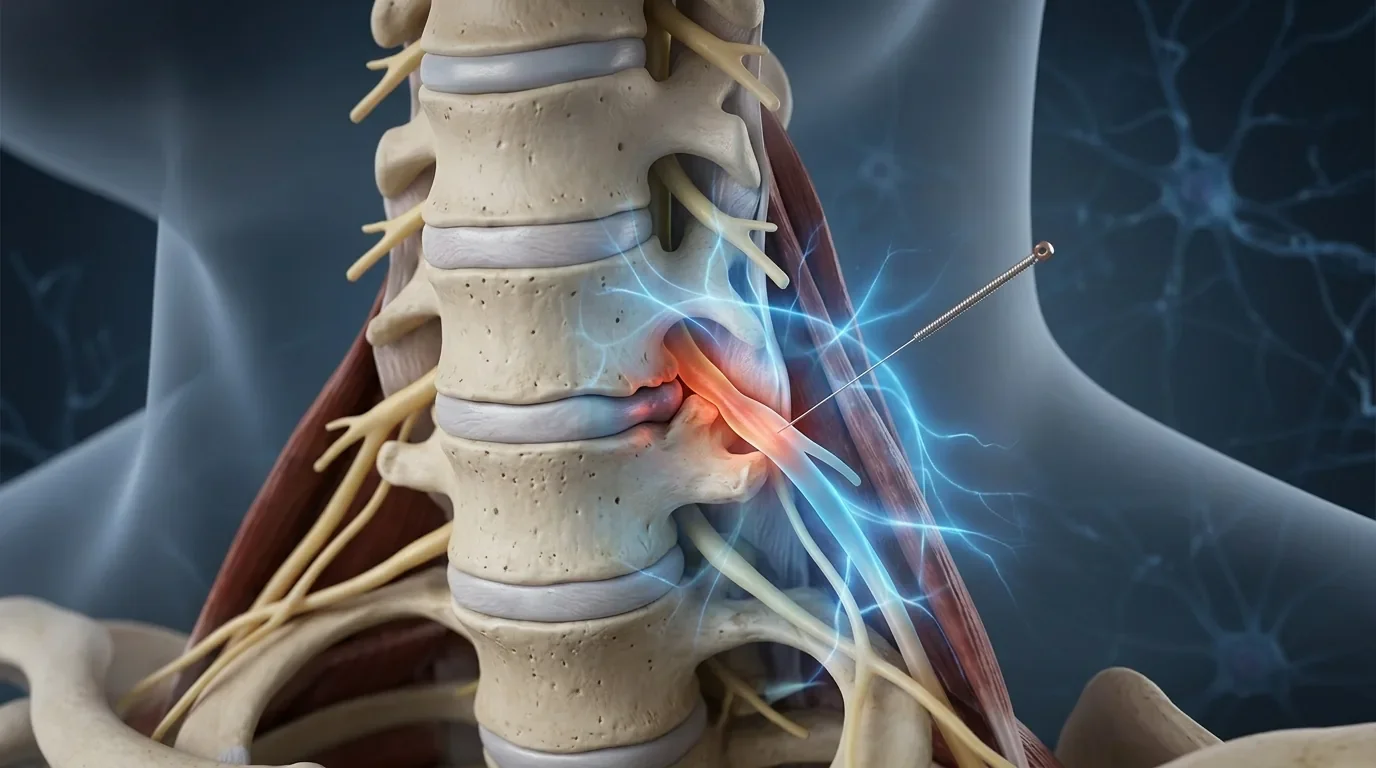
Dry needling is best considered when flares reliably coincide with musculoskeletal drivers: a strip of paraspinal tightness after desk work, QL pain with side-bending, or buttock referral after prolonged sitting. In such cases, hyper-irritable trigger points can refer pain to the lumbosacral region and posterior hip, sustaining a feedback loop of guarding and limited motion.
Treatment uses a thin, solid filiform needle to stimulate targeted neuromuscular tissue. A brief dull ache, localized twitch, or familiar spread toward the belt line or buttock is common during needling and indicates accurate targeting. While a single tight muscle is not responsible for all back pain, addressing muscular input can be materially helpful when paraspinal/hip tension is part of the pattern.
Additional technique context is provided in the Dry Needling Guide.
Back Pain Muscles Considered in Care
When history and examination suggest a muscle-driven component, the following back pain relevant muscles are commonly evaluated. Treatment typically focuses on muscles that reproduce the individual’s referral pattern.
Quadratus lumborum (QL) – often involved in “belt-line” ache and side-bending restrictions; active in prolonged sitting or standing.
Referral pain zone: ipsilateral low back, iliac crest region, and superior gluteal area.
Multifidus – segmental stabilizer prone to guarding with repeated flexion/extension or postural fatigue.
Referral pain zone: deep, localized lumbar ache adjacent to the spine, sometimes with perceived stiffness.
Iliocostalis lumborum and Iliocostalis thoracis – key erector spinae components that flare with prolonged posture or load spikes.
Referral pain zone: longitudinal bands along the lumbar/thoracolumbar column; may echo into the upper buttock.
Erector spinae (thoracolumbar) – global extensor group contributing to palpable “cords” and end-of-day tightness.
Referral pain zone: broad strip of paraspinal discomfort, sometimes wrapping to posterior ribs.
Gluteus medius and Gluteus minimus – lateral hip stabilizers that overload with prolonged standing or walking, or pelvic control deficits.
Referral pain zone: posterolateral hip and buttock; may mimic “sciatic-like” ache without true radicular signs.
Piriformis – deep external rotator sensitive to prolonged sitting or rapid load changes.
Referral pain zone: deep buttock; may project to the posterior thigh in select patterns.
Psoas major – hip flexor that contributes to a lumbar “compressive” feel with prolonged sitting or repetitive flexion.
Referral pain zone: anterior hip/groin with secondary perception of lumbar tightness.
Selection is individualized. Muscles are palpated for taut bands and localized tenderness, then matched against the person’s symptom map. Initial sessions typically address a small, high-yield subset to keep dosing comfortable and clarify what drives change.
Explanations for these muscles are available in the Trigger Points Guide.
What to Expect in a Session (Comfort, Pacing, Soreness)
A typical visit begins with a concise review of symptom frequency/pattern, triggers, activity and position tolerance, and any warning signs that a flare is beginning. Lumbar and hip motion are checked, followed by targeted palpation to identify taut bands and reproduction of familiar referral. The examination informs which muscles are addressed first and how many sites are suitable for the initial appointment.
During needling, a spreading ache or brief twitch may be noticed; these responses tend to settle within seconds. Depending on patient sensitivity, there may be gradual progression over time.
Post-session soreness commonly feels workout-like and can last 24–72 hours. Simple after-care—hydration and comfortable mobility—usually keeps this predictable and brief.
An overview of session flow and common responses appears in the Dry Needling Guide.
Relief Timeline & Visit Cadence
Early change—such as reduced belt-line tightness, fewer warning twinges on bending, or easier rotation—is often reported within 1–3 sessions.
To influence overall frequency or intensity, a short series of approximately 4–6 sessions is common.
Chronic patterns, particularly with long-standing muscular contributors or frequent flares, may require 10 or more visits or ongoing care at a lower maintenance frequency. Spacing is adjusted to sensitivity and schedule (weekly or slightly longer intervals are typical).
Progress is tracked against meaningful markers: number of “bad days,” reliance on short-term relief, or post-flare recovery time. If these metrics are unchanged after a 3–5 session practical trial, treatment variables are adjusted (e.g., alternate muscle priorities, dosing, or visit spacing) or further evaluation is considered.
Dry Needling for Back Pain Research
Systematic Review: Dry Needling for Acute and Chronic Low Back Pain (2023)
This systematic review analyzed meta-analyses and randomized controlled trials published between 2000 and 2023, concluding that dry needling is an effective procedure for treating myofascial pain in patients with both acute and chronic low back pain.
Compared to other modalities such as acupuncture, laser therapy, and physical therapy, dry needling showed superior reduction in post-intervention pain intensity and disability in multiple studies. The review emphasized dry needling’s low risk, minimal invasiveness, and potential utility for patients with medication restrictions; see this broad overview of dry needling for low back pain dry needling for myofascial low back pain systematic review.
Short-Term Effect of Dry Needling for Chronic Mechanical Low Back Pain (2024)
This randomized controlled trial compared the effects of acupuncture dry needling and exercise-based therapy in 30 adults with chronic mechanical low back pain. After treatment, the dry needling group demonstrated significantly greater improvements in lumbar flexion and extension range of motion, as well as larger reductions in pain intensity and disability versus exercise-only controls. The findings suggest that a short series of dry needling sessions can rapidly decrease pain severity and improve functional mobility in chronic low back pain cases. For the full protocol and result breakdown, see this clinical trial on dry needling for mechanical low back pain dry needling clinical trial for mechanical low back pain.
Dry Needling vs Lumbar Spine Mobilization for Chronic Low Back Pain (2025)
This single-blind clinical trial compared dry needling to lumbar spine mobilization in patients with nonspecific chronic low back pain. Both treatments significantly reduced pain and improved functional outcomes, but dry needling showed equivalent or greater improvements in trigger point-related symptoms, pain pressure thresholds, and disability scores.
The results support integrating dry needling for back pain management, especially when trigger points and muscle tension are involved; review protocol comparisons and key results in dry needling vs spine mobilization for chronic low back pain.
Dry Needling of the Gluteus Medius Combined With Standard Physical Therapy for Chronic Low Back Pain (2025)
A randomized, prospective, sham-controlled trial investigated the clinical benefit of adding deep dry needling to the gluteus medius muscle during standard active physical therapy for patients with chronic nonspecific low back pain. Those receiving dry needling showed significantly greater reductions in pain scores and disability levels (Oswestry index), as well as improved lumbar flexion range of motion, compared to controls.
Results also indicated larger improvements among participants with moderate disability, supporting targeted dry needling for the gluteus medius as an evidence-based adjunct to physical therapy for persistent back pain. For direct study details, protocol information, and clinical outcomes, see this controlled trial of dry needling for chronic low back pain dry needling gluteus medius physical therapy trial.
Frequently Asked Questions (FAQ)
Can dry needling help with back pain?
It can be helpful when a muscle-driven component is evident—e.g., consistent paraspinal or hip-stabilizer tension that precedes or accompanies flares and is reproducible on examination. In such cases, reducing trigger-point activity may lower the mechanical input that aggravates symptoms.
How many sessions are needed before results are clear?
A practical trial is 3–5 sessions. Some individuals notice change sooner, while others require a short series to shift frequency or intensity. If progress is not observable in tracked metrics, treatment variables are revised accordingly.
Ready to Try Acupuncture & Dry Needling?
Whether you’re struggling with acute or chronic pain, acupuncture and dry needling may help restore mobility and reduce pain - quickly and safely.
📍 Conveniently located in New York City
🧠 Experts in trigger point therapy, acupuncture, and dry needling
Book your appointment today with the experts at Morningside Acupuncture, the top-rated acupuncture and dry needling clinic in New York City.
Let us help you move better, feel stronger, and live pain-free.
Additional Resources & Next Steps
Learn More: Visit our Blog for further insights into our treatment approach.
What to Expect: During your initial consultation, we perform a comprehensive evaluation to develop a personalized treatment plan.
Patient Stories: Read testimonials from patients who have experienced lasting relief.
Research spotlight: 2024 study—acupuncture & dry needling for chronic low back pain; dry needling for low back pain research summary.
Sources:
Ferreira, G. L., & Sato, J. R. (2023). Treating myofascial pain with dry needling: a systematic review for low back pain. Pain Reports, 8(6), e10756779. https://pmc.ncbi.nlm.nih.gov/articles/PMC10756779/
Alrawaili, S. M., Elshiwi, A. M., Sulieman, A., Azab, A. R., Ezzat, W., Abdelbasset, W. K., & Koura, G. M. (2024). Short-term effect of acupuncture dry needle in treatment of chronic mechanical low back pain: a randomized controlled clinical trial. European Review for Medical and Pharmacological Sciences, 28(14), 3973-3981. https://pubmed.ncbi.nlm.nih.gov/39081147/
Alghadir, A., et al. (2025). The Effect of Dry Needling Compared to Lumbar Spine Mobilization on Functional Disability in Patients with Nonspecific Chronic Low Back Pain. Journal of Back and Musculoskeletal Rehabilitation, 38(4), 789–797. https://pubmed.ncbi.nlm.nih.gov/40958926/
Shulman, L. M., et al. (2025). Dry needling of the gluteus-medius muscle, combined with standard care of active physical therapy in patients with chronic nonspecific low back pain: A randomized, prospective, sham-controlled trial. Journal of Spine Research, 11, Article e12459158. https://pmc.ncbi.nlm.nih.gov/articles/PMC12459158/
Disclaimer: This web site is intended for educational and informational purposes only. Reading this website does not constitute providing medical advice or any professional services. This information should not be used for diagnosing or treating any health issue or disease. Those seeking medical advice should consult with a licensed physician. Seek the advice of a medical doctor or other qualified health professional for any medical condition. If you think you have a medical emergency, call 911 or go to the emergency room. No acupuncturist-patient relationship is created by reading this website or using the information. Morningside Acupuncture PLLC and its employees and contributors do not make any express or implied representations with respect to the information on this site or its use.
Read more from our blog