Pain and the Immune System
Pain and Immune System Infographic
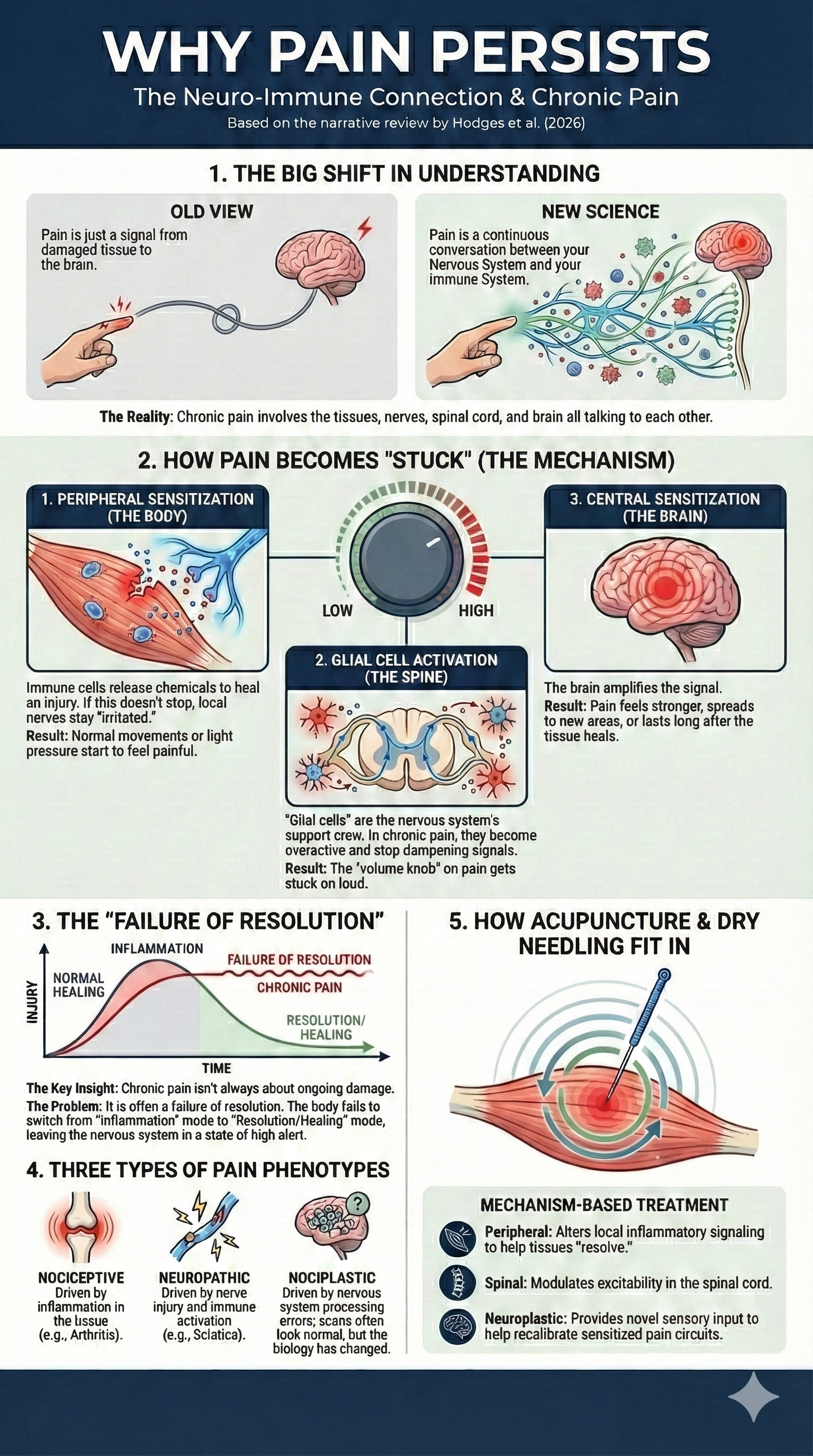
How Neuroinflammation Drives Chronic Pain
Chronic pain is no longer understood as a problem of irritated nerves alone. Over the past two decades, research has shown that pain emerges from ongoing communication between the nervous system and the immune system. This interaction influences how pain starts, how long it lasts, and why it can persist even after tissues appear healed.
A newly published narrative review by Hodges and colleagues (2026) brings this evolving picture into focus, describing chronic pain as a neuro-immune condition involving peripheral tissues, nerves, the spinal cord, and the brain. This article breaks down the key findings of that review and explains what they mean for real-world pain care, including how acupuncture and dry needling may fit into a mechanism-based treatment approach.
Key Points
Chronic pain reflects bidirectional signaling between immune cells and neurons, not just tissue damage.
Neuroinflammation can occur at multiple levels: peripheral tissues, nerves, dorsal root ganglia, spinal cord, and brain.
Different pain types (nociceptive, neuropathic, nociplastic) show distinct neuro-immune patterns.
Pain persistence is increasingly linked to failed inflammatory resolution, not simply ongoing inflammation.
Mechanism-based treatments that influence immune-nervous system interactions may better match individual pain presentations.
What This Research Means for People in Pain
| Scientific Concept | What It Means in Plain English | Why It Matters for Pain |
|---|---|---|
| Neuro-immune interaction | Your nerves and immune system are constantly talking to each other | Pain isn’t just coming from damaged tissue — it’s shaped by ongoing biological signaling |
| Neuroinflammation | Inflammatory activity inside nerves, the spinal cord, or the brain | Pain can persist even after an injury heals because the nervous system stays “irritated” |
| Peripheral sensitization | Pain-sensing nerves in the body become easier to trigger | Normal movements or light pressure may start to feel painful |
| Central sensitization | The spinal cord and brain amplify pain signals | Pain can feel stronger, spread wider, or last longer than expected |
| Glial cell activation | Support cells in the nervous system become overactive | These cells can maintain pain by increasing nerve excitability |
| Failed inflammatory resolution | Inflammation doesn’t fully shut off after it’s no longer needed | Pain becomes chronic not because inflammation continues, but because it never fully resolves |
| Nociplastic pain | Pain driven more by nervous system processing than tissue damage | Scans may look “normal” even though pain is very real |
| Mechanism-based treatment | Choosing treatments based on what’s driving the pain | Matching the treatment to the biology may improve outcomes |
Plain English Breakdown: What’s Actually Going On in Chronic Pain
When people think about pain, they often picture a simple chain reaction: tissue gets injured, nerves send a signal, and the brain feels pain. What this research shows is that the reality is far more interactive and ongoing.
Your nervous system and immune system are constantly communicating. When tissue is injured or stressed, immune cells release chemical signals meant to protect and repair the area. Those same signals also affect nearby pain-sensing nerves, making them more sensitive. In the short term, that sensitivity is useful. It encourages rest and healing. The problem begins when those signals don’t fully turn off.
Over time, pain-sensing nerves in the body can become easier to activate. Movements, pressure, or workloads that used to feel normal may start to trigger pain. This process is often called peripheral sensitization, but in everyday terms it means the volume knob on the pain system has been turned up at the tissue and nerve level.
As pain signals continue to travel toward the spinal cord and brain, additional changes can occur. Support cells in the nervous system, called glial cells, may become overactive. Instead of calming the system, they can amplify incoming signals and reduce the normal inhibitory mechanisms that help dampen pain. This creates a situation where the nervous system becomes more reactive overall.
At this stage, pain is no longer just a message from injured tissue. The spinal cord and brain can begin to magnify pain signals, a process often described as central sensitization. Pain may feel stronger than expected, spread beyond the original area, or linger long after tissues appear healed. This helps explain why imaging studies can look “normal” while pain remains very real and disruptive.
One of the most important ideas from this research is that chronic pain may reflect a failure of resolution rather than ongoing damage. Inflammation is supposed to rise and then settle. When the body does not fully engage its anti-inflammatory and pro-resolving pathways, the nervous system can remain stuck in a heightened state of alert. Pain, in this context, becomes a long-term pattern rather than a short-term warning signal.
This framework also helps explain nociplastic pain, where pain is driven primarily by nervous system processing rather than structural injury. It does not mean the pain is imagined or psychological. It means the biology of the nervous system itself has changed.
The takeaway is that effective pain care often requires more than targeting a single tissue or structure. Treatments that help regulate immune signaling, calm nervous system excitability, and restore normal input over time may be better suited for complex or long-standing pain conditions.
From Neurocentric to Neuro-Immune Models of Pain
Early pain models emphasized neuronal firing as the primary driver of pain. However, landmark research in neuroimmunology demonstrated that immune signaling plays an essential role in modulating nociceptor sensitivity and central pain processing.
Immune mediators such as cytokines, chemokines, prostaglandins, and reactive oxygen species can alter how pain-sensing neurons respond to mechanical, thermal, and chemical stimuli. These effects are not limited to injury sites. Instead, immune-neural signaling extends along the entire pain pathway.
The Hodges et al. review frames pain as a systems-level process, shaped by continuous feedback between immune cells, glial cells, and neurons.
Neuroinflammation Across the Pain Pathway
Peripheral Tissues
In injured or overloaded tissues, immune activation increases local sensitivity through:
Nociceptor activation
Release of inflammatory mediators
Vasodilation and edema
Recruitment of immune cells
This process is adaptive in the short term but becomes problematic when resolution fails.
Peripheral Nerves and DRG
Inflammatory signaling can:
Increase C-fiber excitability
Disrupt myelin integrity
Alter blood–nerve barrier permeability
At the dorsal root ganglia, immune-neural crosstalk may amplify pain signals before they even reach the spinal cord.
Spinal Cord and Brain
Within the central nervous system, activated glial cells (microglia and astrocytes):
Increase synaptic excitability
Reduce inhibitory signaling
Promote maladaptive plasticity
Neuroimaging and molecular studies in humans now support the presence of central neuroinflammation in chronic pain states, especially those without clear structural injury.
| Level | Neuro-Immune Process | Pain Implication |
|---|---|---|
| Peripheral tissues | Immune mediator release, nociceptor sensitization | Local pain amplification |
| Peripheral nerves / DRG | Increased excitability, barrier disruption | Signal amplification before spinal entry |
| Spinal cord | Glial activation, reduced inhibition | Central sensitization |
| Brain | Neuroinflammation, plastic changes | Persistent and nociplastic pain |
Pain Phenotypes and Immune Signaling
Neuropathic Pain
Nerve injury triggers immune activation that can spread along the neuraxis. Feedback loops between neurons and immune cells may sustain pain long after the original insult.
Inflammatory Nociceptive Pain
Conditions such as osteoarthritis and rheumatoid arthritis often begin with tissue-driven inflammation but may gradually involve central neuroimmune mechanisms.
Nociplastic Pain
In nociplastic conditions, immune signaling within the central nervous system appears to play a prominent role, even when peripheral pathology is minimal or absent.
Pain Chronicity as a Failure of Resolution
One of the most important concepts highlighted in the review is that chronic pain may result from insufficient engagement of anti-inflammatory and pro-resolving pathways.
Immune responses are not inherently harmful. Early inflammation supports healing. Problems arise when:
Pro-inflammatory signaling persists
Anti-inflammatory cytokines (such as IL-10) are under-expressed
Pro-resolving mediators fail to terminate the inflammatory response
This imbalance promotes long-term sensitization and maladaptive nervous system plasticity.
Translational Challenges and Human Evidence
Much mechanistic data comes from animal models, which cannot fully replicate human pain complexity. Still, growing human evidence supports neuroimmune involvement in chronic pain, including:
Tissue-level immune changes
Transcriptomic shifts in pain pathways
PET imaging markers of glial activation
These findings reinforce the need for treatments aligned with dominant mechanisms rather than one-size-fits-all approaches.
Where Acupuncture and Dry Needling May Fit In
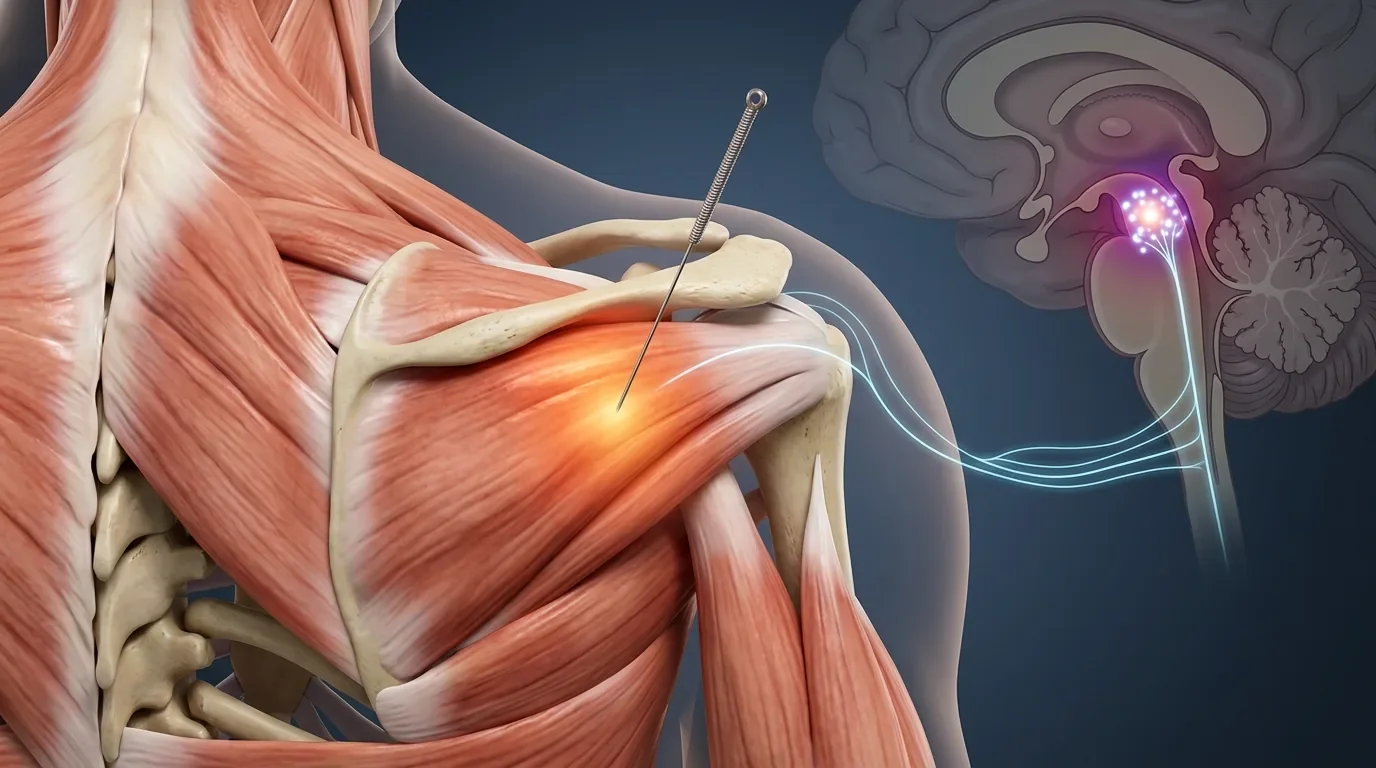
Acupuncture and dry needling use acupuncture needles to mechanically and neurophysiologically influence tissue, nerve, and central signaling. While techniques vary, several mechanisms discussed in neuroimmune pain research may be relevant:
Peripheral Immune Modulation
Needle insertion can influence local inflammatory signaling by:
Altering nociceptor input
Affecting neuropeptide release
Modifying local immune cell behavior
This may help shift tissue environments away from sustained pro-inflammatory states.
Spinal and Supraspinal Effects
Research suggests acupuncture may modulate spinal excitability and descending inhibitory pathways, which interact closely with glial and immune signaling within the central nervous system.
Neuroplastic Regulation
By altering afferent input patterns, acupuncture and dry needling may contribute to recalibration of sensitized neural circuits over time, especially when combined with movement, exercise, and load management.
Importantly, these effects are best understood as regulatory rather than curative. In chronic pain, repeated inputs that reduce excessive excitability and support resolution may be more meaningful than short-term symptom suppression.
Clinical Takeaway
Pain should be viewed less as a static diagnosis and more as a dynamic neuro-immune state. Treatments that acknowledge this complexity, including acupuncture and dry needling, may be most effective when integrated into a broader plan that addresses movement, stress physiology, sleep, and immune regulation.
Frequently Asked Questions (FAQ)
Is chronic pain always inflammatory?
Not always, but immune signaling plays a role in many chronic pain states, even when overt inflammation is not visible.
Does this mean pain is “all in the immune system”?
No. Pain emerges from interactions between immune activity, neural processing, biomechanics, and psychosocial factors.
Can acupuncture reduce neuroinflammation?
Research suggests acupuncture may influence immune-neural signaling, but effects vary by condition and individual response.
Ready to Try Acupuncture & Dry Needling?
Whether you’re struggling with acute or chronic pain, acupuncture and dry needling may help restore mobility and reduce pain - quickly and safely.
📍 Conveniently located in New York City
🧠 Experts in trigger point therapy, acupuncture, and dry needling
Book your appointment today with the experts at Morningside Acupuncture, the top-rated acupuncture and dry needling clinic in New York City.
Let us help you move better, feel stronger, and live pain-free.
Additional Resources & Next Steps
Learn More: Visit our Blog for further insights into our treatment approach.
What to Expect: During your initial consultation, we perform a comprehensive evaluation to develop a personalized treatment plan.
Patient Stories: Read testimonials from patients who have experienced lasting relief.
Sources:
Hodges, P. W., et al. (2026). Neuro-immune mechanisms in chronic pain: Implications for mechanism-based treatment. Pain Reports. https://www.sciencedirect.com/science/article/pii/S2468781225002322
Watkins, L. R., & Maier, S. F. (2002). Beyond neurons: Evidence that immune and glial cells contribute to pathological pain states. Physiological Reviews, 82(4), 981–1011. https://pubmed.ncbi.nlm.nih.gov/12270950/
Ji, R. R., Nackley, A., Huh, Y., Terrando, N., & Maixner, W. (2018). Neuroinflammation and central sensitization in chronic pain. Anesthesiology, 129(2), 343–366. https://pubmed.ncbi.nlm.nih.gov/36775098/
Disclaimer: This web site is intended for educational and informational purposes only. Reading this website does not constitute providing medical advice or any professional services. This information should not be used for diagnosing or treating any health issue or disease. Those seeking medical advice should consult with a licensed physician. Seek the advice of a medical doctor or other qualified health professional for any medical condition. If you think you have a medical emergency, call 911 or go to the emergency room. No acupuncturist-patient relationship is created by reading this website or using the information. Morningside Acupuncture PLLC and its employees and contributors do not make any express or implied representations with respect to the information on this site or its use. For any legal interpretation of scope of practice in your state, consult a licensed attorney or regulatory authority.
Read more from our blog