Best Acupuncture Points for Knee Pain
The "Eyes of the Knee," GB34, BL40, and the Thigh Muscle Trigger Points That Acupuncture Points at the Knee Are Often Targeting
Acupuncture for knee pain uses a combination of points directly at the joint, points on the thigh that address the muscles loading the knee, and distal points on the leg that activate supraspinal pain inhibition. Understanding these three layers makes the treatment selection for arthritis, tendinopathy, and runner's knee much clearer.
- Acupuncture for osteoarthritis of the knee has been studied extensively, with the Acupuncture Trialists' Collaboration finding clinically meaningful pain reduction and functional improvement compared to sham and usual care, with effect sizes that are clinically relevant for daily function (Vickers et al., 2018).
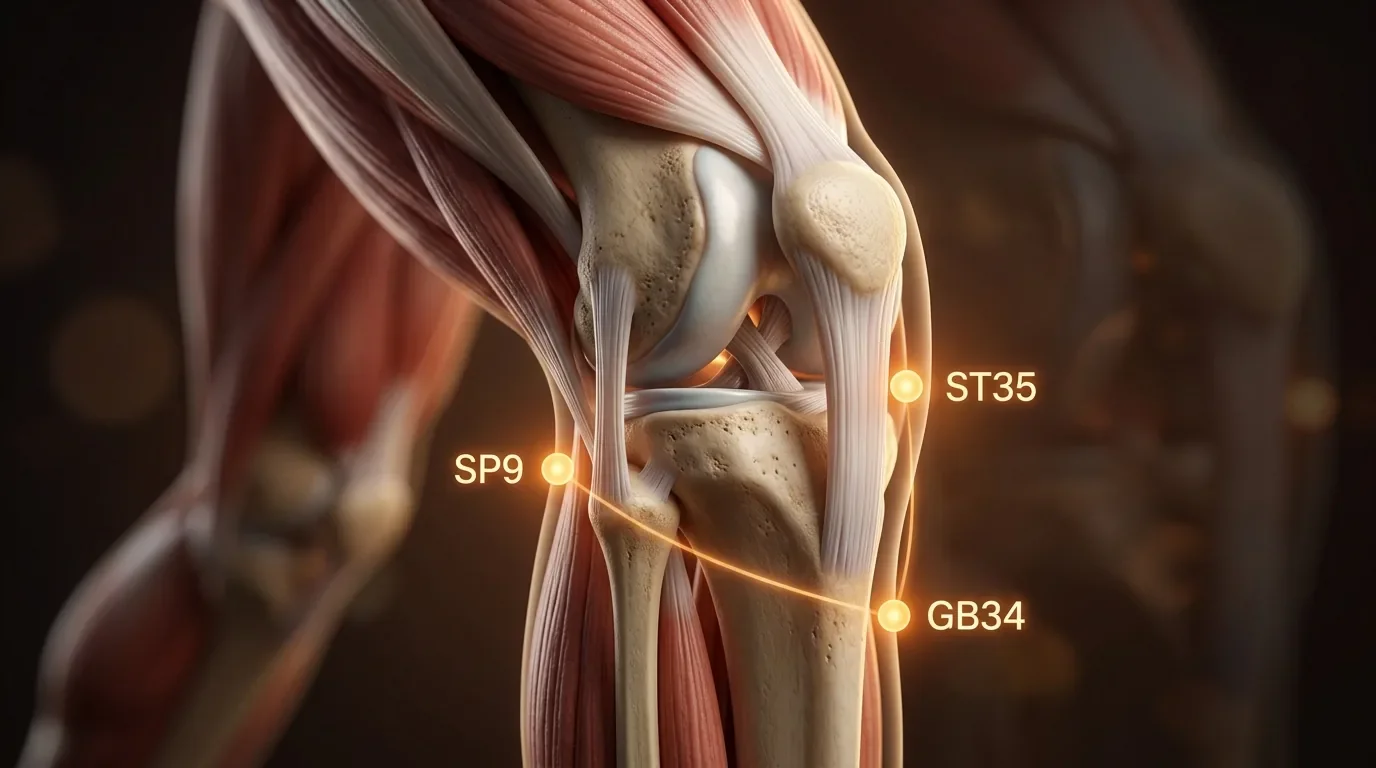
- The "eyes of the knee," ST35 and EX-LE5 (Xiyan), are the two depressions flanking the patellar ligament in the flexed knee; they provide direct access to the joint capsule, infrapatellar fat pad, and synovial membrane, and needling them is among the most reliably anti-inflammatory local approaches for intraarticular knee pain.
- GB34 (Yanglingquan), located anterior and inferior to the fibular head on the lateral leg, is classified as the meeting point of the sinews in classical acupuncture and is used for all musculoskeletal conditions regardless of location; at the knee it is particularly useful for IT band syndrome, lateral compartment pain, and fibular head tenderness.
- Most knee pain has a significant referred component from quadriceps trigger points, particularly rectus femoris and vastus medialis, and several knee acupuncture points are selected specifically for their access to these muscles rather than the joint itself (Simons et al., 1999).
- BL40 in the popliteal fossa, while primarily used for low back pain, is also a core point for posterior knee pain and is used in all general knee pain protocols for its supraspinal descending inhibition effect.
- SP10 (Xuehai) on the medial thigh, 2 cun above the medial superior border of the patella, is positioned over the vastus medialis oblique (VMO), whose weakness and inhibition is one of the most common causes of patellar tracking problems and medial knee pain in runners and desk workers alike.
Is knee pain limiting your stairs, your runs, or your daily walking?
Knee pain responds to acupuncture when treatment addresses both the local joint environment and the muscle loading patterns that are stressing it. Our practitioners evaluate which quadriceps muscles and hip stabilizers are involved in your knee presentation and tailor the point selection accordingly.
Schedule NowThe Knee as a Downstream Problem: Why Hip and Thigh Muscles Matter
Knee pain is often a downstream consequence of problems further up the kinetic chain. Vastus medialis inhibition allows the patella to track laterally, producing patellofemoral syndrome. Rectus femoris trigger points refer pain directly to the anterior knee and mimic patellar tendinopathy. TFL and gluteus medius weakness allow the femur to internally rotate and adduct during weight-bearing, increasing valgus stress at the knee. Popliteus trigger points refer pain into the posterior knee in patterns consistent with posterior meniscus injury.
This is why acupuncture point selection for knee pain extends well beyond the knee joint itself. Points on the medial thigh access the vastus medialis; points at the fibular head address the IT band insertion and biceps femoris; points in the gluteal region reduce the hip muscle inhibition that is stressing the knee per step. The joint-level points are important for local inflammation and intraarticular pain, but the thigh and hip points address the load distribution problem that produced the joint inflammation in the first place (Simons et al., 1999).
Related Dry Needling for Knee Pain: Quadriceps Trigger Points and Patellar TrackingKey Acupuncture Points for Knee Pain
| Point | Anatomical Location | Target Tissue | Clinical Use |
|---|---|---|---|
| ST35 / EX-LE5 (Xiyan) | Lateral and medial depressions flanking the patellar ligament when the knee is flexed at 90° | Joint capsule; infrapatellar fat pad; synovial membrane | Osteoarthritis, patellofemoral syndrome, joint swelling, intraarticular pain; the primary local points for the knee joint itself |
| GB34 (Yanglingquan) | Anterior and inferior to the head of the fibula, in the depression between the fibula and the tibialis anterior | Peroneus longus origin; fibular head region; deep peroneal nerve | Lateral knee pain, IT band syndrome, fibular head tenderness, musculoskeletal pain generally; meeting point of sinews |
| SP10 (Xuehai) | 2 cun above the medial superior border of the patella, over the bulge of vastus medialis oblique | Vastus Medialis (VMO); medial femoral territory | Patellar tracking disorders, medial knee pain, quadriceps inhibition; key for patellofemoral syndrome |
| SP9 (Yinlingquan) | Medial knee, in the depression below and behind the medial condyle of the tibia | Posterior medial tibia; sartorial fascia; medial gastrocnemius origin | Medial knee pain, posteromedial knee aching, fluid accumulation; strong local point for the medial compartment |
| BL40 (Weizhong) | Midpoint of the popliteal fossa, between biceps femoris and semitendinosus tendons | Posterior knee fascia; tibial nerve; popliteal vessels | Posterior knee pain, popliteus tenderness, general knee pain; distal point for supraspinal inhibition |
| ST34 (Liangqiu) | 2 cun above the lateral superior border of the patella, on the vastus lateralis | Vastus Lateralis; rectus femoris tendon | Acute knee pain, quadriceps tension, patellofemoral syndrome; xi-cleft point, used for acute conditions |
| LV8 (Ququan) | Medial end of the knee crease when flexed, anterior to the semimembranosus and semitendinosus tendons | Medial joint line; medial knee ligament territory; Sartorius distal region | Medial joint line pain, medial meniscus irritation, inner knee aching; also for adductor referred knee pain |
| ST36 (Zusanli) | 3 cun below ST35, 1 cun lateral to the anterior tibial crest, over the tibialis anterior | Tibialis anterior; deep peroneal nerve; anterior compartment | Distal analgesic and anti-inflammatory; general knee pain and osteoarthritis; vagal activation; one of the most broadly used points in all of acupuncture |
GB34 and the Lateral Knee: More Than Just an IT Band Point
GB34 (Yanglingquan) is one of the most important points in the acupuncture system for musculoskeletal conditions because of its classical designation as the "meeting point of the sinews" — a concept that, in neurophysiological terms, may reflect the point's location at a convergence of several important anatomical structures. The fibular head region houses the peroneus longus origin, the insertion of the biceps femoris, the lateral collateral ligament attachment, and the common peroneal nerve as it wraps around the fibular neck. Stimulating GB34 in the dense connective tissue at this convergence activates multiple afferent nerve pathways simultaneously and produces analgesic effects across a broad musculoskeletal territory.
For knee pain specifically, GB34 is most useful for lateral compartment pain, IT band syndrome where tightness presents at the fibular head, biceps femoris tendon irritation, and any knee pain that is worse on lateral movement or stair descent. It is typically combined with local points at the knee in every treatment, regardless of the specific presentation, because its supraspinal modulation effect and its local influence on the lateral knee tissue make it a broadly applicable and reliable choice.
Related Rectus Femoris Trigger Points: Knee Pain and Quadriceps Tension Related Popliteus Trigger Points: Posterior Knee Pain and LockingIs knee pain from arthritis or running injuries limiting your activities?
Both osteoarthritic knee pain and overuse injuries like runner's knee and patellar tendinopathy respond to acupuncture treatment that addresses the local joint environment and the muscle load patterns that are stressing it. Our practitioners at Morningside evaluate the full presentation to select the combination of local, thigh-level, and distal points that fit your specific pattern.
Schedule NowAcupuncture for Knee Osteoarthritis: What the Evidence Shows
Knee osteoarthritis is one of the most researched conditions in acupuncture clinical trials. The consistent finding across multiple large randomized controlled trials and meta-analyses is that acupuncture produces clinically meaningful reductions in pain and improvements in function for knee OA, with effects that are larger than sham acupuncture and significantly larger than no treatment, and that persist at follow-up periods of six to twelve months (Vickers et al., 2018). These findings led major rheumatology and orthopedic guidelines, including the American College of Rheumatology guidelines for osteoarthritis management, to conditionally recommend acupuncture for knee OA.
The mechanism is multifactorial. Local needling at the knee joint reduces intraarticular inflammatory cytokine concentrations, an effect documented in synovial fluid analysis after acupuncture. The segmental spinal cord modulation at the L3–L4 levels, which supply the knee, reduces central sensitization that amplifies the pain signal from arthritic joint surfaces. The supraspinal descending inhibition activated by points like BL40 and ST36 provides systemic pain modulation. Together, these mechanisms reduce the pain of arthritis without modifying the underlying structural joint change, but in a way that meaningfully improves daily function for most patients.
Ready to take the next step toward less knee pain and more activity?
At Morningside Acupuncture, we are the highest-rated acupuncture and dry needling clinic in New York City with over 500 five-star Google reviews. We treat knee pain from osteoarthritis, patellar tendinopathy, IT band syndrome, meniscus irritation, and post-surgical recovery. Our combination of local acupuncture points, thigh muscle trigger point work, and distal point selection is tailored to the specific structures involved in your knee presentation.
Schedule NowFrequently Asked Questions
Can acupuncture help knee pain from osteoarthritis?
Yes. Acupuncture for knee osteoarthritis is supported by multiple large clinical trials and is conditionally recommended in several major clinical guidelines. The treatment does not reverse articular cartilage loss, but it reduces pain and improves function through local anti-inflammatory effects, spinal cord pain modulation, and supraspinal descending inhibition. Most patients with knee OA experience meaningful improvement in daily pain and walking tolerance within four to six sessions.
Which acupuncture points are most important for runner's knee?
Patellofemoral syndrome (runner's knee) primarily involves patellar tracking problems from vastus medialis weakness and vastus lateralis tightness. The most important points are SP10 over the VMO, ST34 over the vastus lateralis, and the eyes of the knee for local joint treatment. Hip-level points targeting the gluteus medius are often added to address the femoral internal rotation that stresses the patellofemoral joint, particularly in runners with hip drop during their stride.
How is acupuncture for knee pain different from cortisone injection?
Cortisone injections reduce intraarticular inflammation rapidly and powerfully but have limited duration and may weaken tendon and cartilage tissue with repeated use. Acupuncture produces more modest local anti-inflammatory effects but also addresses the muscle load patterns and pain sensitization that cortisone cannot reach. The two treatments are not mutually exclusive, and some patients use acupuncture as a way to extend the benefit of injections and address the surrounding muscle dysfunction that cortisone leaves untreated.
Does acupuncture hurt at the knee?
Needling at the eyes of the knee (ST35 and EX-LE5) typically produces a local aching or pressure sensation as the needle enters the joint capsule area. This is expected and tolerable for most patients. Points like SP10 over the vastus medialis or GB34 at the fibular head may produce a referred sensation into the knee or leg when they contact trigger point tissue. Distal points are generally well-tolerated.
References
- Vickers, A. J., Vertosick, E. A., Lewith, G., MacPherson, H., Foster, N. E., Sherman, K. J., ... & Acupuncture Trialists' Collaboration. (2018). Acupuncture for chronic pain: Update of an individual patient data meta-analysis. The Journal of Pain, 19(5), 455–474. https://doi.org/10.1016/j.jpain.2017.11.005
- Zhao, Z. Q. (2008). Neural mechanism underlying acupuncture analgesia. Progress in Neurobiology, 85(4), 355–375. https://doi.org/10.1016/j.pneurobio.2008.05.004
- Simons, D. G., Travell, J. G., & Simons, L. S. (1999). Travell & Simons' Myofascial Pain and Dysfunction: The Trigger Point Manual (2nd ed.). Williams & Wilkins.
- Yarnitsky, D. (2010). Conditioned pain modulation (the diffuse noxious inhibitory control-like effect): Its relevance for acute and chronic pain states. Current Opinion in Anaesthesiology, 23(5), 611–615. https://doi.org/10.1097/ACO.0b013e32833c348b
- Kolasinski, S. L., Neogi, T., Hochberg, M. C., Oatis, C., Guyatt, G., Block, J., ... & Reston, J. (2020). 2019 American College of Rheumatology/Arthritis Foundation guideline for the management of osteoarthritis of the hand, hip, and knee. Arthritis & Rheumatology, 72(2), 220–233. https://doi.org/10.1002/art.41142
Disclaimer: This web site is intended for educational and informational purposes only. Reading this website does not constitute providing medical advice or any professional services. This information should not be used for diagnosing or treating any health issue or disease. Those seeking medical advice should consult with a licensed physician. Seek the advice of a medical doctor or other qualified health professional for any medical condition. If you think you have a medical emergency, call 911 or go to the emergency room. No acupuncturist-patient relationship is created by reading this website or using the information. Morningside Acupuncture PLLC and its employees and contributors do not make any express or implied representations with respect to the information on this site or its use. For any legal interpretation of scope of practice in your state, consult a licensed attorney or regulatory authority.
Read more from our blog