Best Acupuncture Points for Sciatica
The Bladder Meridian Pathway and Key Points Along the Sciatic Nerve's Course: GB30, BL36, BL40, BL57, and BL60 for Buttock, Thigh, and Leg Pain
Sciatica describes pain that travels along the course of the sciatic nerve from the buttock down the posterior leg, and the primary acupuncture points for it are selected to follow that same anatomical pathway. This post explains why the bladder meridian line and the sciatic nerve run parallel, and how needling at each of the key points along that route addresses the different aspects of sciatic pain.
- The posterior leg pathway of the bladder meridian channel in classical acupuncture closely corresponds to the anatomical course of the sciatic nerve, which explains why bladder meridian points from the gluteal region to the ankle have historically been the primary acupuncture selections for sciatic pain.
- Sciatica has at least two distinct mechanisms that require different acupuncture approaches: disc-related nerve root compression at the lumbar spine, in which local lumbar and sacral points provide segmental nerve root modulation, and piriformis-related sciatic nerve entrapment in the buttock, in which GB30 provides direct access to the compressing muscle (Simons et al., 1999).
- GB30 (Huantiao) is the single most important point for sciatic pain because it is placed directly over the piriformis muscle and adjacent to the sciatic nerve as it exits below the piriformis, allowing the needle to address both the muscular compression and the nerve irritation simultaneously.
- The clinical literature on acupuncture for low back pain with radiation into the leg, which encompasses most sciatica presentations, shows significant improvements in pain intensity and disability compared with sham acupuncture and conventional treatment alone (Vickers et al., 2018).
- Central sensitization is a major component of chronic sciatica: the dorsal horn neurons at L4–S1 become hyperexcitable after prolonged nerve irritation, and systemic points like BL40 and ST36 that activate supraspinal descending inhibition are essential for addressing this central component alongside the peripheral compression.
- Acupuncture for sciatica is generally more effective when combined with assessment and treatment of the lumbar trigger points and movement patterns that are contributing to the disc or piriformis compression, rather than being applied as a pain modulation tool in isolation.
Is sciatic pain shooting into your leg and making sitting or driving unbearable?
Sciatica that does not resolve with rest often involves a combination of peripheral nerve compression and central pain sensitization that acupuncture can address from multiple directions simultaneously. Our practitioners at Morningside evaluate the full pattern of sciatic pain, from the compression source to the distal symptom distribution, to select the most targeted combination of local and systemic points.
Schedule NowWhy the Bladder Meridian Points Follow the Sciatic Nerve
One of the more clinically useful observations about the classical bladder meridian channel is that its posterior leg pathway runs almost exactly along the course of the sciatic nerve and its major branches. The sciatic nerve exits the pelvis below or through the piriformis muscle (at the location of GB30), crosses the gluteal region (BL36 area), runs down the posterior thigh (BL36–BL40), passes through the popliteal fossa (BL40), divides into the tibial and peroneal nerves, and continues to the ankle and foot (BL57, BL60). Needling along this pathway provides direct access to the nerve and the muscles surrounding it at each level, which is why the bladder meridian is the primary acupuncture channel for sciatic presentations.
From a neurophysiological perspective, needling at points along this pathway produces afferent signals in the same spinal cord segments that receive input from the irritated sciatic nerve. This segmental convergence creates inhibitory effects at the dorsal horn that reduce the pain signal arriving from the nerve root or peripheral nerve compression site. The distal points also activate supraspinal systems, producing a descending inhibitory state that reduces the hyperexcitability of the entire L4–S1 spinal segment (Zhao, 2008).
Related Sciatica Treatment in NYC: Acupuncture and Dry Needling ApproachesKey Acupuncture Points for Sciatica
| Point | Anatomical Location | Nerve / Tissue Access | Clinical Role |
|---|---|---|---|
| BL23 / BL25 (Lumbar) | 1.5 cun lateral to L2 and L4 spinous processes respectively | Erector spinae at L2 and L4; dorsal rami of L2 and L4 | Segmental nerve root modulation at the disc levels most commonly involved in disc-related sciatica (L4–L5, L5–S1 nearby) |
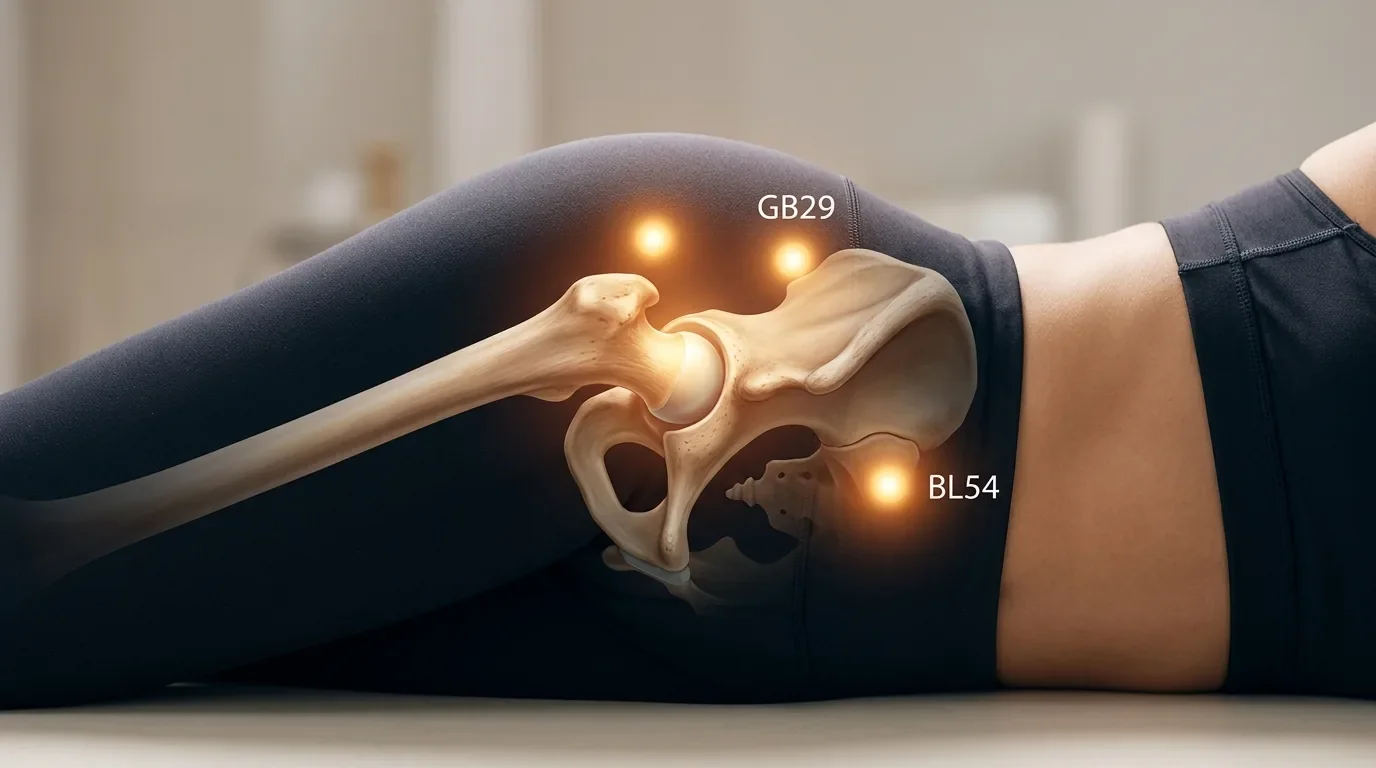
| BL54 (Zhibian) | 3 cun lateral to the sacral hiatus (GV3 level) | Gluteus maximus; sacral nerve roots; inferior gluteal nerve | Sacral root modulation; used for sciatica with sacral origin or S1–S2 root irritation; combined with GB30 for comprehensive gluteal coverage |
| GB30 (Huantiao) | Junction of outer third and inner two-thirds of the trochanter-to-sacral-hiatus line | Piriformis; sciatic nerve exit point; gluteus maximus | Primary point for sciatic nerve pain; addresses piriformis compression directly; produces de qi that may radiate along the sciatic pathway to the foot |
| BL36 (Chengfu) | Midpoint of the gluteal crease, below the ischial tuberosity | Posterior thigh; sciatic nerve in the posterior thigh; Biceps Femoris | Mid-point along the sciatic nerve pathway; used for sciatica extending into the posterior thigh; also for hamstring pain and ischial tuberosity tenderness |
| BL40 (Weizhong) | Midpoint of the popliteal fossa, between biceps femoris and semitendinosus tendons | Tibial nerve; popliteal fascia; popliteal vessels | Command point for back and leg; addresses sciatic nerve at the posterior knee level; activates supraspinal descending inhibition; essential for all sciatica protocols |
| BL57 (Chengshan) | Midline of the posterior calf, at the apex of the gastrocnemius muscle belly junction | Gastrocnemius; tibial nerve; soleus adjacent | Distal point for sciatic pain extending into the calf; also addresses calf cramping that often accompanies sciatica; tibial nerve territory at S1–S2 |
| BL60 (Kunlun) | Depression between the posterior lateral malleolus and the Achilles tendon | Sural nerve; peroneal tendons; Achilles tendon lateral border | Distal point at the ankle level of the sciatic pathway; used for pain extending to the foot and ankle; anti-inflammatory for Achilles tendinopathy component |
| GB34 (Yanglingquan) | Anterior and inferior to the fibular head | Common peroneal nerve (lateral sciatic division); peroneus longus | Addresses peroneal nerve branch of sciatic; used when sciatica presents with lateral leg pain, foot drop component, or fibular head tenderness |
Disc-Related Sciatica vs. Piriformis Syndrome: Different Emphases
The point selection for sciatica shifts depending on whether the primary compression is at the lumbar disc level or at the piriformis in the hip. Both produce similar symptom distributions down the posterior leg, but they differ in the presence of lumbar pain, the behavior of symptoms with flexion versus extension, and the response to certain provocative tests.
Disc-related sciatica, in which a herniated disc is compressing the L4, L5, or S1 nerve root, responds best to local lumbar points (BL23, BL25, BL32) combined with the full lower-extremity pathway points (GB30, BL40, BL57, BL60). The local lumbar needling provides segmental nerve root modulation at the compressed level, while the distal pathway points reduce central sensitization and provide supraspinal pain inhibition. This combination is supported by research showing that acupuncture significantly reduces pain and disability in lumbar radiculopathy presentations (Vickers et al., 2018).
Piriformis syndrome, in which the sciatic nerve is compressed or irritated by a hypertonic or shortened piriformis muscle rather than by a disc, shifts the emphasis to GB30 and trigger point treatment of the piriformis and the surrounding gluteal muscles. The lumbar points are less central because the compression is peripheral rather than spinal, though they are still included to address the secondary spinal sensitization that often develops after prolonged sciatic nerve irritation.
Related Piriformis Trigger Points: Sciatic Nerve Compression and Buttock Pain Related Dry Needling for Sciatica: Piriformis Syndrome and Lumbar Trigger PointsHas sciatica been interfering with your daily life for weeks or months?
Chronic sciatica that has not responded to rest, NSAIDs, or physical therapy alone often has both a peripheral compression component and a central sensitization component that acupuncture can address simultaneously. Our practitioners combine local gluteal and lumbar needling with the full sciatic pathway point sequence and distal analgesic points to address the full picture of sciatic pain. We also work with patients who have imaging-confirmed disc herniations alongside conservative care.
Schedule NowFrequently Asked Questions
Is acupuncture effective for sciatica from a herniated disc?
Research supports acupuncture for lumbar radiculopathy, which is the term for nerve root compression from disc herniation that produces sciatica. Acupuncture does not remove the herniation, but it can reduce the pain by modulating the nerve root irritation at the segmental level and reducing the central sensitization that amplifies the radiating pain. Most patients with disc-related sciatica notice meaningful improvement in pain and function within four to eight sessions.
Can acupuncture help sciatica that goes all the way to the foot?
Yes. The distal bladder meridian points BL57 and BL60 specifically address the pain that extends into the calf and foot, corresponding to the S1 and S2 nerve root distributions that supply the lateral calf and plantar foot. For sciatica with foot involvement, the full pathway from GB30 through BL60 is typically used in each session, along with GB34 at the fibular head for any lateral leg or foot drop component.
How many sessions does acupuncture for sciatica typically take?
Acute sciatica from a recent disc event or piriformis flare often responds significantly within three to five sessions, with rapid reduction of acute pain followed by progressive functional improvement. Chronic sciatica that has been present for months to years, particularly if there is significant central sensitization, typically requires eight to twelve sessions with ongoing maintenance sessions as needed. Your response after the first two to three treatments gives a strong indication of your likely trajectory.
Does needling GB30 hurt?
GB30 requires a deep needle placement to reach the piriformis, and many patients experience a strong de qi sensation that may radiate down the leg. This radiation along the sciatic pathway is expected and is not the same as pain, though it can feel dramatic when it occurs. Most patients tolerate GB30 well once they understand what the sensation means. The sensation typically subsides within seconds and is often followed by a sense of warmth or relief in the buttock and thigh.
References
- Vickers, A. J., Vertosick, E. A., Lewith, G., MacPherson, H., Foster, N. E., Sherman, K. J., ... & Acupuncture Trialists' Collaboration. (2018). Acupuncture for chronic pain: Update of an individual patient data meta-analysis. The Journal of Pain, 19(5), 455–474. https://doi.org/10.1016/j.jpain.2017.11.005
- Zhao, Z. Q. (2008). Neural mechanism underlying acupuncture analgesia. Progress in Neurobiology, 85(4), 355–375. https://doi.org/10.1016/j.pneurobio.2008.05.004
- Simons, D. G., Travell, J. G., & Simons, L. S. (1999). Travell & Simons' Myofascial Pain and Dysfunction: The Trigger Point Manual (2nd ed.). Williams & Wilkins.
- Cherkin, D. C., Sherman, K. J., Avins, A. L., Erro, J. H., Ichikawa, L., Barlow, W. E., ... & Deyo, R. A. (2009). A randomized trial comparing acupuncture, simulated acupuncture, and usual care for chronic low back pain. Archives of Internal Medicine, 169(9), 858–866. https://doi.org/10.1001/archinternmed.2009.214
- Yarnitsky, D. (2010). Conditioned pain modulation (the diffuse noxious inhibitory control-like effect): Its relevance for acute and chronic pain states. Current Opinion in Anaesthesiology, 23(5), 611–615. https://doi.org/10.1097/ACO.0b013e32833c348b
Disclaimer: This web site is intended for educational and informational purposes only. Reading this website does not constitute providing medical advice or any professional services. This information should not be used for diagnosing or treating any health issue or disease. Those seeking medical advice should consult with a licensed physician. Seek the advice of a medical doctor or other qualified health professional for any medical condition. If you think you have a medical emergency, call 911 or go to the emergency room. No acupuncturist-patient relationship is created by reading this website or using the information. Morningside Acupuncture PLLC and its employees and contributors do not make any express or implied representations with respect to the information on this site or its use. For any legal interpretation of scope of practice in your state, consult a licensed attorney or regulatory authority.
Read more from our blog