Sphincter Ani Trigger Points
Pelvic floor trigger points
Introduction
The sphincter ani is a circular muscle of the anus responsible for bowel control, continence, and pelvic stability. When trigger points develop in this muscle, they can cause rectal pain, pelvic floor tightness, and difficulty with bowel movements, often mimicking hemorrhoids, pelvic floor dysfunction, or proctalgia fugax (rectal spasms).
Name and Area
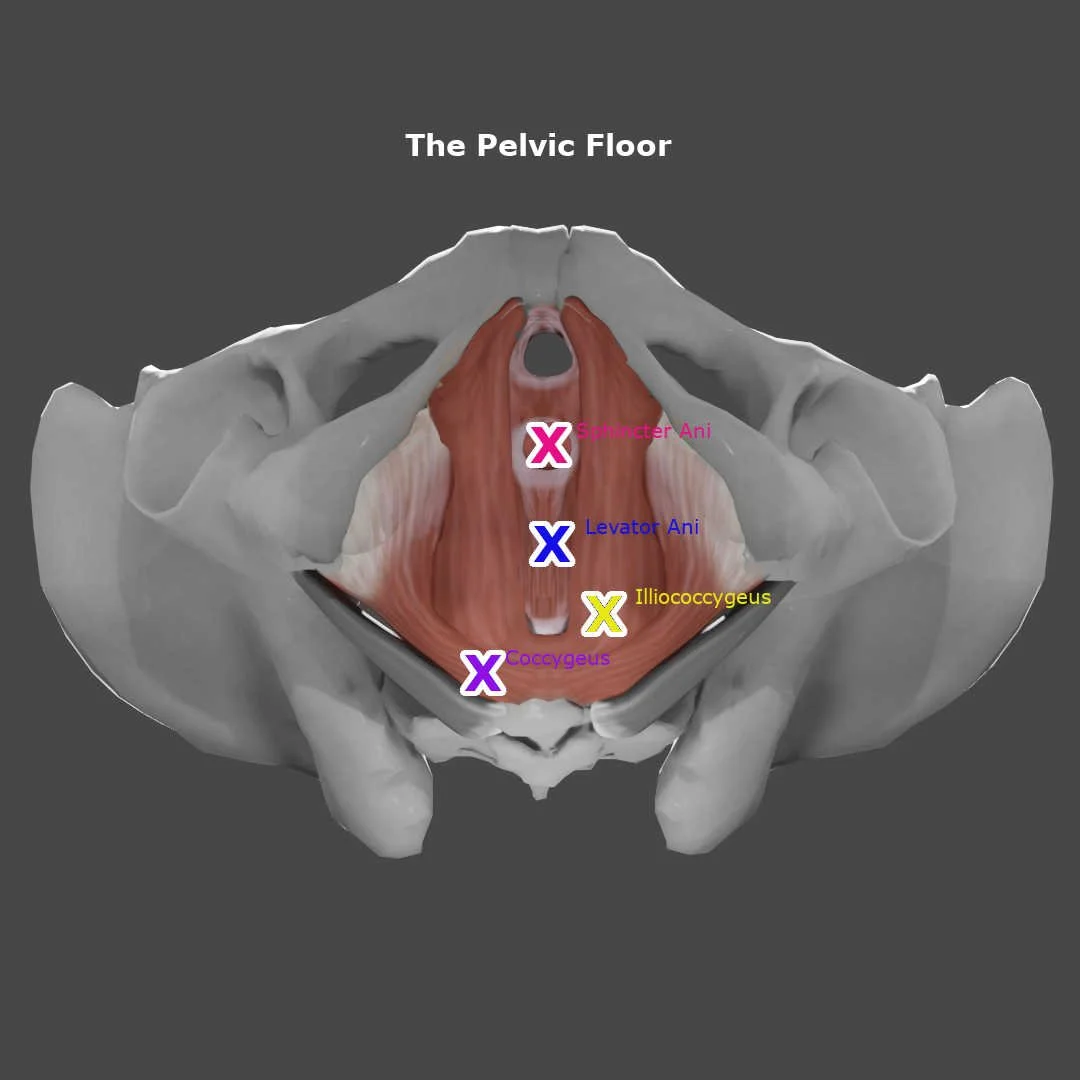
Name: Sphincter Ani (External and Internal)
Area: Located around the anus, forming part of the pelvic floor and lower digestive tract.
Indications
Sphincter ani trigger points may contribute to:
Pain in the rectum or around the anus (mistaken for hemorrhoids or anal fissures)
Pain that extends to the perineum and tailbone (can mimic pudendal neuralgia or SI joint dysfunction)
Rectal spasms or a sudden "cramping" sensation (common in proctalgia fugax and pelvic floor dysfunction)
Pain or discomfort when sitting for long periods (common in cyclists, office workers, and postpartum individuals)
Difficulty or painful bowel movements (can resemble IBS, constipation, or anal sphincter dysfunction)
Increased sensitivity or pain after sexual activity (common in those with pelvic floor hypertonicity)
Pain from this muscle is often mistaken for hemorrhoids, IBS, or chronic pelvic pain syndrome.
Muscle Action
Controls Bowel Movements: Maintains continence by tightening or relaxing the anal opening.
Supports the Pelvic Floor: Works with other pelvic muscles to maintain stability and posture.
Assists in Reflexive Responses: Involves autonomic and voluntary control for bowel regulation.
The sphincter ani is essential for bowel function, pelvic stability, and overall continence.
Signs and Symptoms
Individuals with sphincter ani trigger points often report:
Pain or discomfort in the anus and rectum that feels like a dull ache or cramping
Sudden, brief rectal spasms that occur at night (common in proctalgia fugax)
Pain that radiates to the tailbone, perineum, or lower pelvic region
Difficulty with bowel movements, including constipation or painful straining
Pain or sensitivity that worsens with sitting, cycling, or sexual activity
Discomfort that feels like a "pressure" in the rectum, even when there’s no need to defecate
Pain worsens with prolonged sitting, stress, or pelvic floor dysfunction.
Perpetuating Factors
Common causes of sphincter ani trigger points include:
Chronic constipation or straining (can lead to increased muscle tightness and spasms)
Pelvic floor dysfunction (hypertonicity or weakness can affect bowel and bladder control)
Prolonged sitting (common in office workers, truck drivers, and cyclists)
Postpartum recovery or pelvic surgery (can alter pelvic muscle function and cause increased tension)
Emotional stress or anxiety (can increase pelvic muscle tension and trigger painful spasms)
Trigger Point Referral Pattern
Trigger points in the sphincter ani refer pain to:
The anus and rectum (Can Mimic Hemorrhoids, Anal Fissures, or Proctitis)
The perineum and tailbone (Mistaken for Pudendal Neuralgia or Coccydynia)
The lower pelvic floor and sit bones (Can Resemble SI Joint Dysfunction or Pelvic Pain Syndrome)
Pain from this muscle is often confused with digestive issues, nerve entrapment, or postural dysfunction.
Differential Diagnosis
Sphincter ani trigger points may be mistaken for:
Hemorrhoids (swollen veins in the rectum, often with itching or bleeding)
Anal fissures (small tears in the anal lining, cause sharp pain with bowel movements)
Proctalgia fugax (sudden, unexplained rectal spasms that last minutes to hours)
Irritable bowel syndrome (IBS) (abdominal discomfort with bowel movement irregularities)
Pudendal neuralgia (burning or numbness in the pelvic floor, worse when sitting)
A thorough pelvic floor, rectal, and lower back examination is necessary to rule out these conditions.
Associated Trigger Points
Sphincter ani trigger points often co-exist with:
Levator ani (deep pelvic pain, can contribute to rectal and perineal discomfort)
Obturator internus (inner hip and perineal pain, can affect pelvic floor stability)
Gluteus maximus (lower back and buttock pain, affects sitting comfort and pelvic support)
Coccygeus (tailbone pain, common in those with pelvic floor dysfunction or coccydynia)
Anatomy and Innervation
| Muscle | Origin | Insertion | Innervation |
|---|---|---|---|
| External Anal Sphincter | Perineal body, anococcygeal ligament | Skin and fascia around the anus | Pudendal nerve (S2–S4) |
| Internal Anal Sphincter | Circular smooth muscle of the rectum | Skin and fascia around the anus | Autonomic nervous system (Pelvic splanchnic nerves, S2–S4) |
The sphincter ani is innervated by the pudendal nerve and autonomic nervous system, which also control bowel function, pelvic stability, and continence.
Patient Examination
A comprehensive examination should include:
Palpation: Identify tender nodules along the perineum, rectal area, and lower pelvic floor.
Digital Rectal Exam (If Necessary): Assess muscle tightness, spasms, or weakness in the anal sphincter.
Pelvic Floor Muscle Function Testing: Evaluate muscle coordination and tension patterns.
Postural and Sitting Tolerance Assessment: Check for sit bone pressure sensitivity or tailbone pain.
Corrective Actions
Dry Needling
Dry needling can release trigger points in the sphincter ani, reducing rectal tightness and improving pelvic floor function.
Manual Therapy
Trigger Point Release: Apply deep sustained pressure to tight spots in the pelvic floor and perineal muscles.
Myofascial Release: Helps improve circulation and reduce chronic pelvic muscle tension.
Stretching
Deep Squat Stretch: Helps lengthen and relax the pelvic floor muscles.
Happy Baby Pose: Opens the hips and relieves tension in the lower pelvis and perineum.
Strengthening Exercises
Pelvic Floor Relaxation Drills: Focus on controlled diaphragmatic breathing to release excessive tension.
Glute Bridges: Helps engage the posterior chain and support pelvic alignment.
Postural and Lifestyle Adjustments
Avoid prolonged sitting without movement breaks (prevents excessive rectal and pelvic floor tension).
Use proper toileting techniques (avoid straining, engage pelvic muscles properly during bowel movements).
Practice stress management and relaxation techniques (reduces chronic pelvic floor tightness).
Conclusion
The sphincter ani plays a crucial role in bowel control, pelvic stability, and continence, but trigger points in this muscle can cause significant rectal, perineal, and lower pelvic pain. By incorporating dry needling, manual therapy, stretching, and pelvic floor relaxation techniques, individuals can reduce pain, improve function, and prevent chronic rectal discomfort.
➡️ Learn more about Trigger Points
➡️ Explore our Trigger Point Index
Sources:
Travell, J. G., & Simons, D. G. (1983). Myofascial Pain and Dysfunction: The Trigger Point Manual (2nd ed.). Williams & Wilkins.
Simons, D., & Travell, J. (1999). The Trigger Point Manual, Volume 2: The Lower Extremities. Williams & Wilkins.